

Severe Acute Respiratory Syndrome Coronavirus 2 Convalescent Plasma Versus Standard Plasma in Coronavirus Disease 2019 Infected Hospitalized Patients in New York: A Double-Blind Randomized Trial
- PMID: 33870923
- PMCID: PMC9658886
- DOI: 10.1097/CCM.0000000000005066
Severe Acute Respiratory Syndrome Coronavirus 2 Convalescent Plasma Versus Standard Plasma in Coronavirus Disease 2019 Infected Hospitalized Patients in New York: A Double-Blind Randomized Trial
Abstract
Objectives: Four peer-reviewed publications have reported results from randomized controlled trials of convalescent plasma for coronavirus disease 2019 infection; none were conducted in the United States nor used standard plasma as a comparator. To determine if administration of convalescent plasma to patients with coronavirus disease 2019 increases antibodies to severe acute respiratory syndrome coronavirus 2 and improves outcome.
Design: Double-blind randomized controlled trial.
Setting: Hospital in New York.
Patients: Patients with polymerase chain reaction documented coronavirus disease 2019 infection.
Interventions: Patients were randomized (4:1) to receive 2 U of convalescent plasma versus standard plasma. Antibodies to severe acute respiratory syndrome coronavirus 2 were measured in plasma units and in trial recipients.
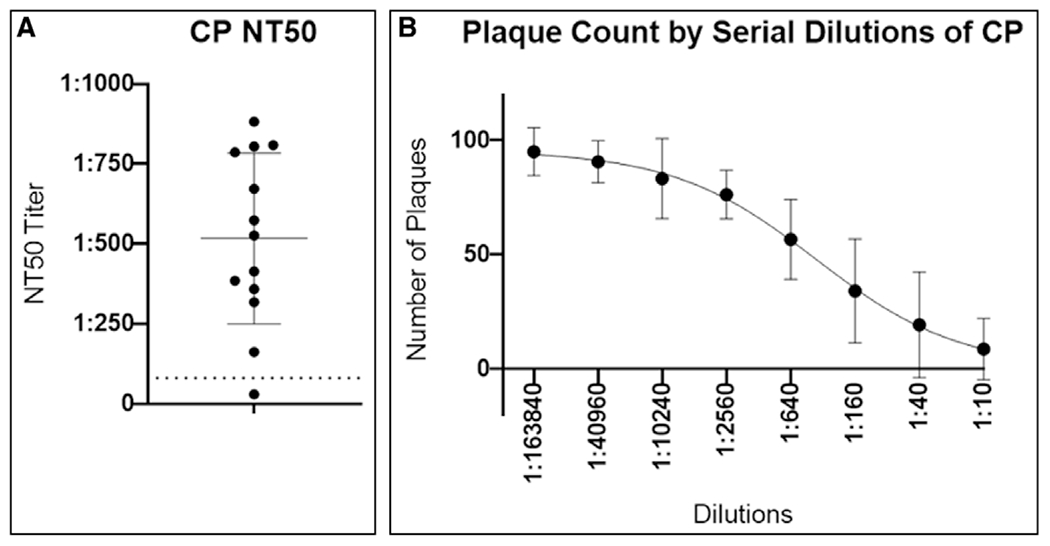
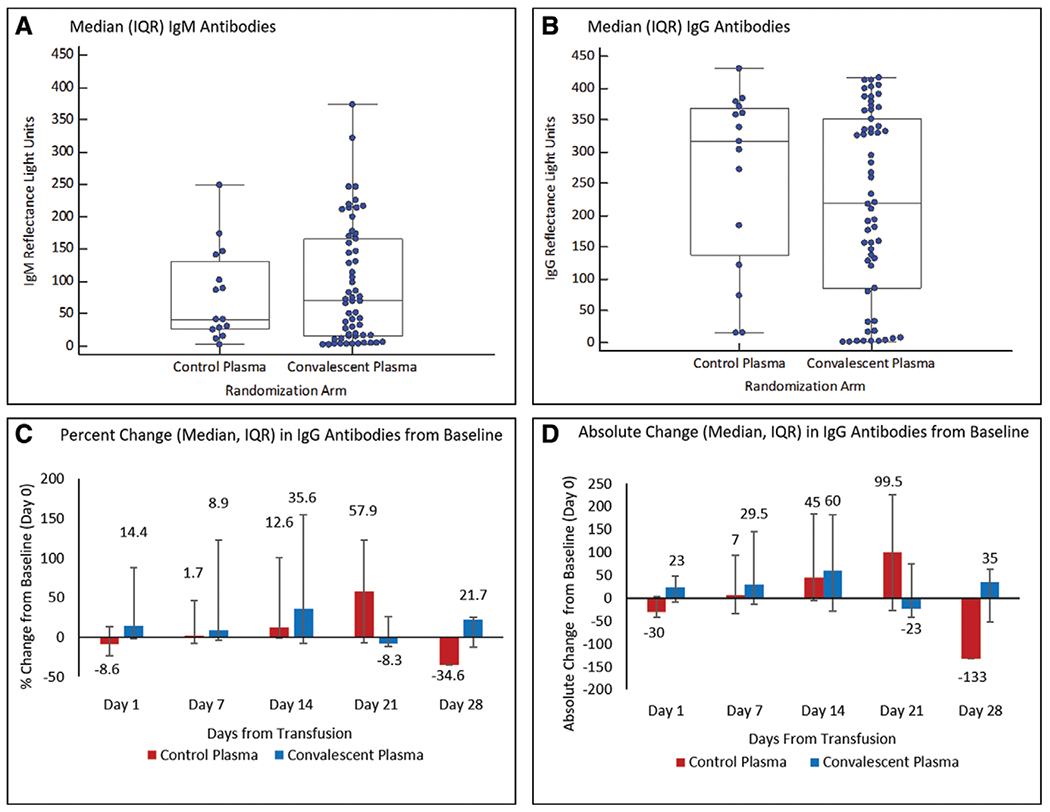
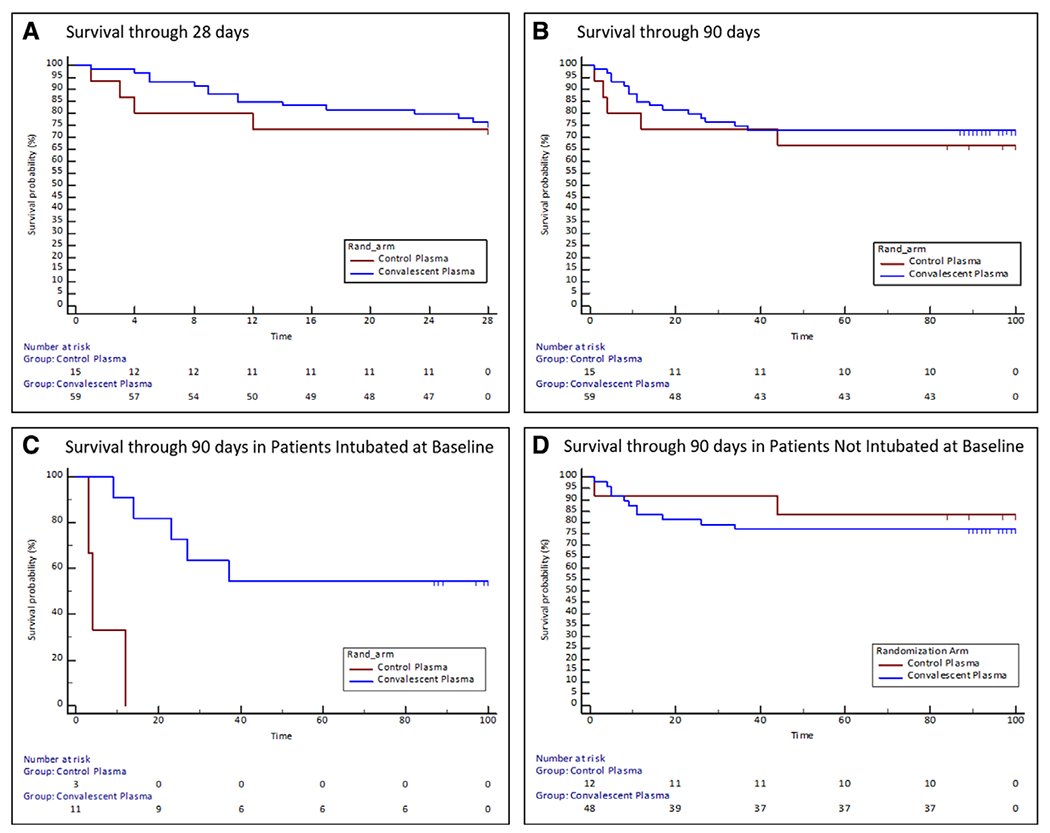
Measurements and main results: Enrollment was terminated after emergency use authorization was granted for convalescent plasma. Seventy-four patients were randomized. At baseline, mean (sd) Acute Physiology and Chronic Health Evaluation II score (23.4 [5.6] and 22.5 [6.6]), percent of patients intubated (19% and 20%), and median (interquartile range) days from symptom onset to randomization of 9 (6-18) and 9 (6-15), were similar in the convalescent plasma versus standard plasma arms, respectively. Convalescent plasma had high neutralizing activity (median [interquartile range] titer 1:526 [1:359-1:786]) and its administration increased antibodies to severe acute respiratory syndrome coronavirus 2 by 14.4%, whereas standard plasma administration led to an 8.6% decrease (p = 0.005). No difference was observed for ventilator-free days through 28 days (primary study endpoint): median (interquartile range) of 28 (2-28) versus 28 (0-28; p = 0.86) for the convalescent plasma and standard plasma groups, respectively. A greater than or equal to 2 point improvement in the World Health Organization scale was achieved by 20% of subjects in both arms (p = 0.99). All-cause mortality through 90 days was numerically lower in the convalescent plasma versus standard plasma groups (27% vs 33%; p = 0.63) but did not achieve statistical significance. A key prespecified subgroup analysis of time to death in patients who were intubated at baseline was statistically significant; however, sample size numbers were small.
Conclusions: Administration of convalescent plasma to hospitalized patients with coronavirus disease 2019 infection increased antibodies to severe acute respiratory syndrome coronavirus disease 2 but was not associated with improved outcome.
Trial registration: ClinicalTrials.gov NCT04344535.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Dr. Fries received support for article research from the National Institutes of Health. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Convalescent Plasma and Coronavirus Disease 2019: Time for Reassessment.Crit Care Med. 2021 Jul 1;49(7):1182-1186. doi: 10.1097/CCM.0000000000005068. Crit Care Med. 2021. PMID: 33870924 No abstract available.
References
-
- Sanders JM, Monogue ML, Jodlowski TZ, et al.: Pharmacologic treatments for coronavirus disease 2019 (COVID-19): A review. JAMA 2020; 323:1824–1836 - PubMed
-
- Mair-Jenkins J, Saavedra-Campos M, Baillie JK, et al.; Convalescent Plasma Study Group: The effectiveness of convalescent plasma and hyperimmune immunoglobulin for the treatment of severe acute respiratory infections of viral etiology: A systematic review and exploratory meta-analysis. J Infect Dis 2015; 211:80–90 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
