

Resuming Training in High-Level Athletes After Mild COVID-19 Infection: A Multicenter Prospective Study (ASCCOVID-19)
- PMID: 35751748
- PMCID: PMC9233721
- DOI: 10.1186/s40798-022-00469-0
Resuming Training in High-Level Athletes After Mild COVID-19 Infection: A Multicenter Prospective Study (ASCCOVID-19)
Abstract
Background: There is a paucity of data on cardiovascular sequelae of asymptomatic/mildly symptomatic SARS-Cov-2 infections (COVID).
Objectives: The aim of this prospective study was to characterize the cardiovascular sequelae of asymptomatic/mildly symptomatic COVID-19 among high/elite-level athletes.
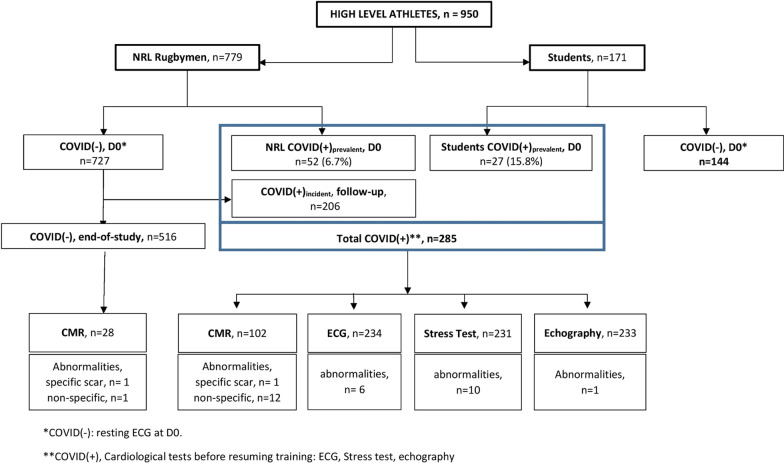
Methods: 950 athletes (779 professional French National Rugby League (F-NRL) players; 171 student athletes) were included. SARS-Cov-2 testing was performed at inclusion, and F-NRL athletes were intensely followed-up for incident COVID-19. Athletes underwent ECG and biomarker profiling (D-Dimer, troponin, C-reactive protein). COVID(+) athletes underwent additional exercise testing, echocardiography and cardiac magnetic resonance imaging (CMR).
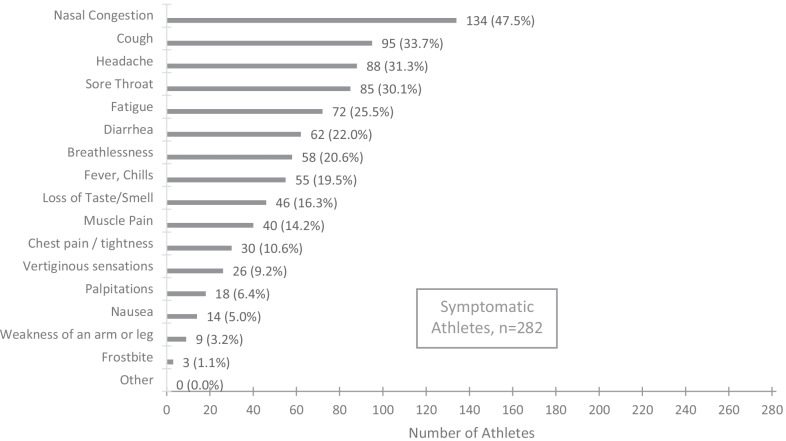
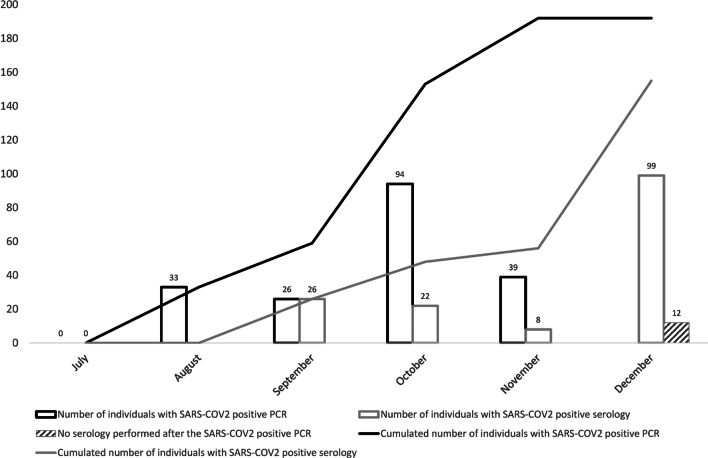
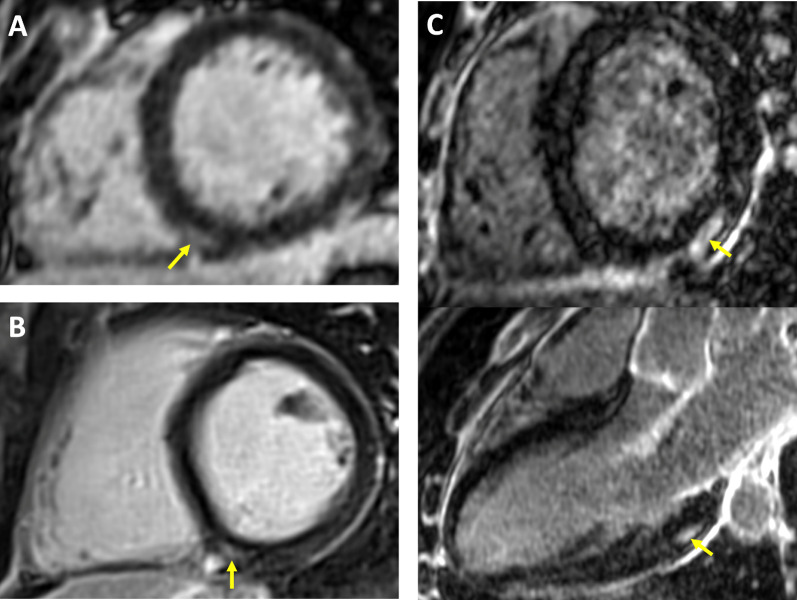
Results: 285/950 athletes (30.0%) had mild/asymptomatic COVID-19 [79 (8.3%) at inclusion (COVID(+)prevalent); 206 (28.3%) during follow-up (COVID(+)incident)]. 2.6% COVID(+) athletes had abnormal ECGs, while 0.4% had an abnormal echocardiogram. During stress testing (following 7-day rest), COVID(+) athletes had a functional capacity of 12.8 ± 2.7 METS with only stress-induced premature ventricular ectopy in 10 (4.3%). Prevalence of CMR scar was comparable between COVID(+) athletes and controls [COVID(+) vs. COVID(-); 1/102 (1.0%) vs 1/28 (3.6%)]. During 289 ± 56 days follow-up, one athlete had ventricular tachycardia, with no obvious link with a SARS-CoV-2 infection. The proportion with troponin I and CRP values above the upper-limit threshold was comparable between pre- and post-infection (5.9% vs 5.9%, and 5.6% vs 8.7%, respectively). The proportion with D-Dimer values above the upper-limit threshold increased when comparing pre- and post-infection (7.9% vs 17.3%, P = 0.01).
Conclusion: The absence of cardiac sequelae in pauci/asymptomatic COVID(+) athletes is reassuring and argues against the need for systematic cardiac assessment prior to resumption of training (clinicaltrials.gov; NCT04936503).
Keywords: Cardiac MRI; ECG; Echocardiography; SARS-CoV-2; Sport; Stress test.
© 2022. The Author(s).
Conflict of interest statement
Abbott has kindly provided the anti-SARS-CoV-2 serology tests (IgG and IgM) to the biology department of the Bordeaux University Hospital (I. Pellegrin, S. Picard, P. Trimoulet) for centralized serologies. The other authors declare that they have no competing interests.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
