

Effectiveness of a Multicomponent Quality Improvement Strategy to Improve Achievement of Diabetes Care Goals: A Randomized, Controlled Trial
- PMID: 27398874
- PMCID: PMC6561084
- DOI: 10.7326/M15-2807
Effectiveness of a Multicomponent Quality Improvement Strategy to Improve Achievement of Diabetes Care Goals: A Randomized, Controlled Trial
Erratum in
-
Correction: Effectiveness of a Multicomponent Quality Improvement Strategy to Improve Achievement of Diabetes Care Goals.Ann Intern Med. 2017 Aug 15;167(4):292. doi: 10.7326/L17-0327. Ann Intern Med. 2017. PMID: 28806811 No abstract available.
Abstract
Background: Achievement of diabetes care goals is suboptimal globally. Diabetes-focused quality improvement (QI) is effective but remains untested in South Asia.
Objective: To compare the effect of a multicomponent QI strategy versus usual care on cardiometabolic profiles in patients with poorly controlled diabetes.
Design: Parallel, open-label, pragmatic randomized, controlled trial. (ClinicalTrials.gov: NCT01212328).
Setting: Diabetes clinics in India and Pakistan.
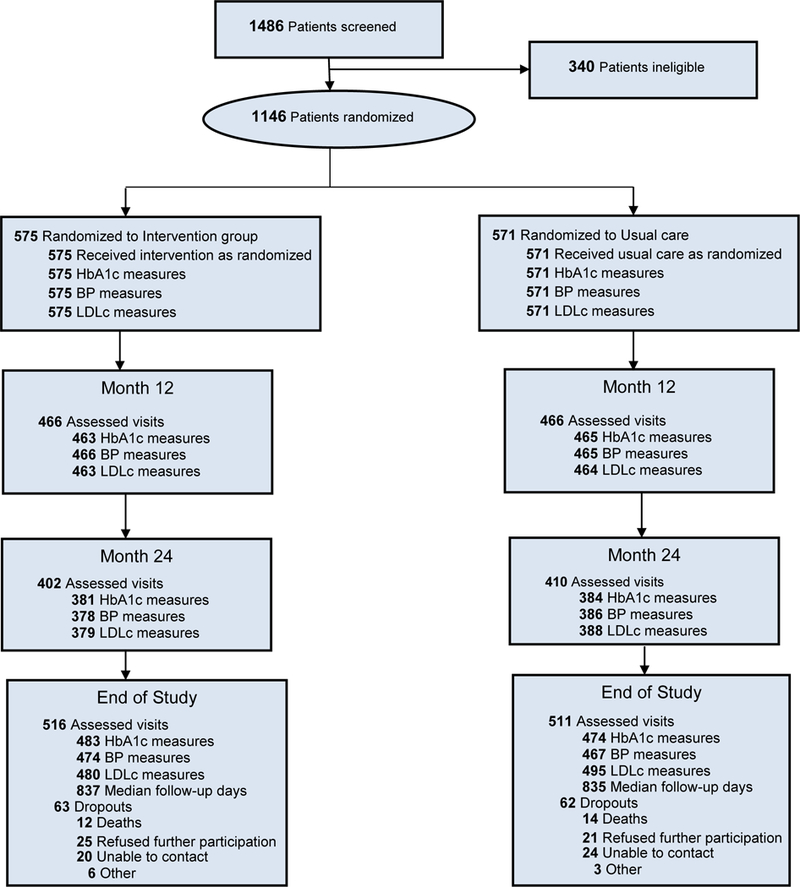
Patients: 1146 patients (575 in the intervention group and 571 in the usual care group) with type 2 diabetes and poor cardiometabolic profiles (glycated hemoglobin [HbA1c] level ≥8% plus systolic blood pressure [BP] ≥140 mm Hg and/or low-density lipoprotein cholesterol [LDLc] level ≥130 mg/dL).
Intervention: Multicomponent QI strategy comprising nonphysician care coordinators and decision-support electronic health records.
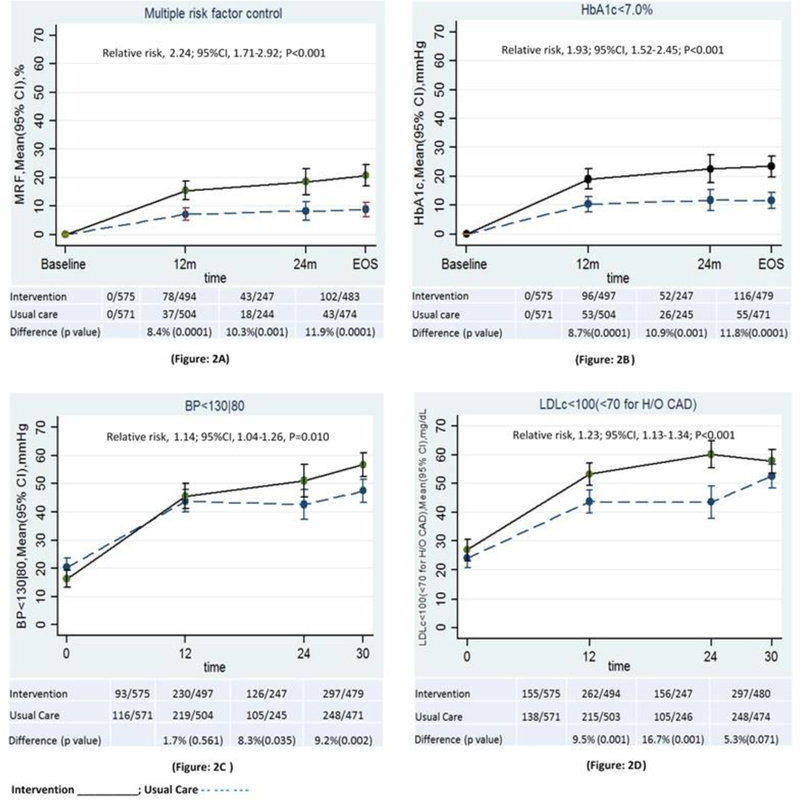
Measurements: Proportions achieving HbA1c level less than 7% plus BP less than 130/80 mm Hg and/or LDLc level less than 100 mg/dL (primary outcome); mean risk factor reductions, health-related quality of life (HRQL), and treatment satisfaction (secondary outcomes).
Results: Baseline characteristics were similar between groups. Median diabetes duration was 7.0 years; 6.8% and 39.4% of participants had preexisting cardiovascular and microvascular disease, respectively; mean HbA1c level was 9.9%; mean BP was 143.3/81.7 mm Hg; and mean LDLc level was 122.4 mg/dL. Over a median of 28 months, a greater percentage of intervention participants achieved the primary outcome (18.2% vs. 8.1%; relative risk, 2.24 [95% CI, 1.71 to 2.92]). Compared with usual care, intervention participants achieved larger reductions in HbA1c level (-0.50% [CI, -0.69% to -0.32%]), systolic BP (-4.04 mm Hg [CI, -5.85 to -2.22 mm Hg]), diastolic BP (-2.03 mm Hg [CI, -3.00 to -1.05 mm Hg]), and LDLc level (-7.86 mg/dL [CI, -10.90 to -4.81 mg/dL]) and reported higher HRQL and treatment satisfaction.
Limitation: Findings were confined to urban specialist diabetes clinics.
Conclusion: Multicomponent QI improves achievement of diabetes care goals, even in resource-challenged clinics.
Primary funding source: National Heart, Lung, and Blood Institute and UnitedHealth Group.
Figures
References
-
- International Diabetes Federation. Diabetes Atlas (2014 Update). 2014.
-
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837–53. - PubMed
-
- The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329(14):977–86. - PubMed
-
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–89. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical