

The impact of the COVID-19 pandemic on antimicrobial usage: an international patient-level cohort study
- PMID: 40151230
- PMCID: PMC11945301
- DOI: 10.1093/jacamr/dlaf037
The impact of the COVID-19 pandemic on antimicrobial usage: an international patient-level cohort study
Abstract
Background: This study aimed to evaluate the trends in antimicrobial prescription during the first 1.5 years of COVID-19 pandemic.
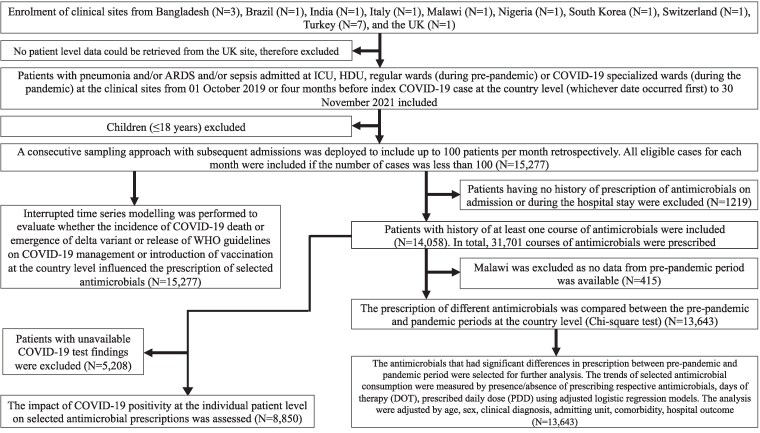
Methods: This was an observational, retrospective cohort study using patient-level data from Bangladesh, Brazil, India, Italy, Malawi, Nigeria, South Korea, Switzerland and Turkey from patients with pneumonia and/or acute respiratory distress syndrome and/or sepsis, regardless of COVID-19 positivity, who were admitted to critical care units or COVID-19 specialized wards. The changes of antimicrobial prescription between pre-pandemic and pandemic were estimated using logistic or linear regression. Pandemic effects on month-wise antimicrobial usage were evaluated using interrupted time series analyses (ITSAs).
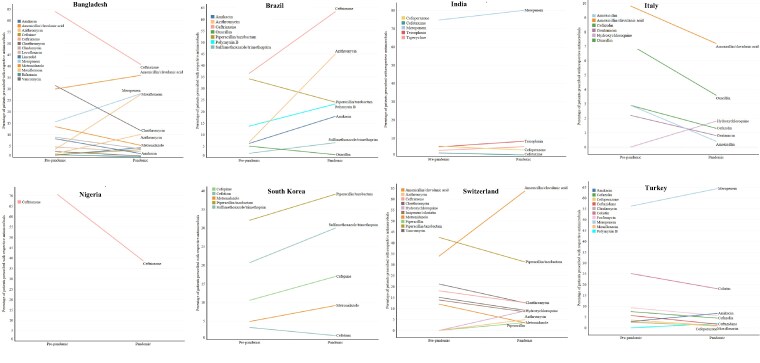
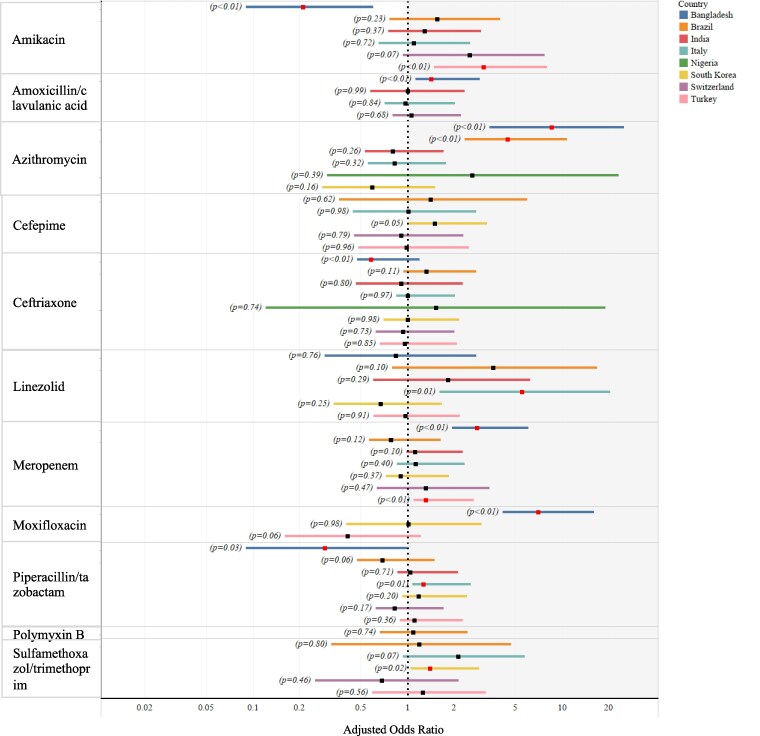
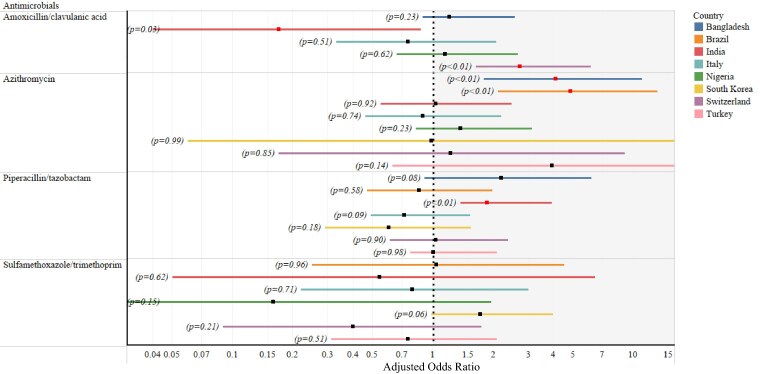
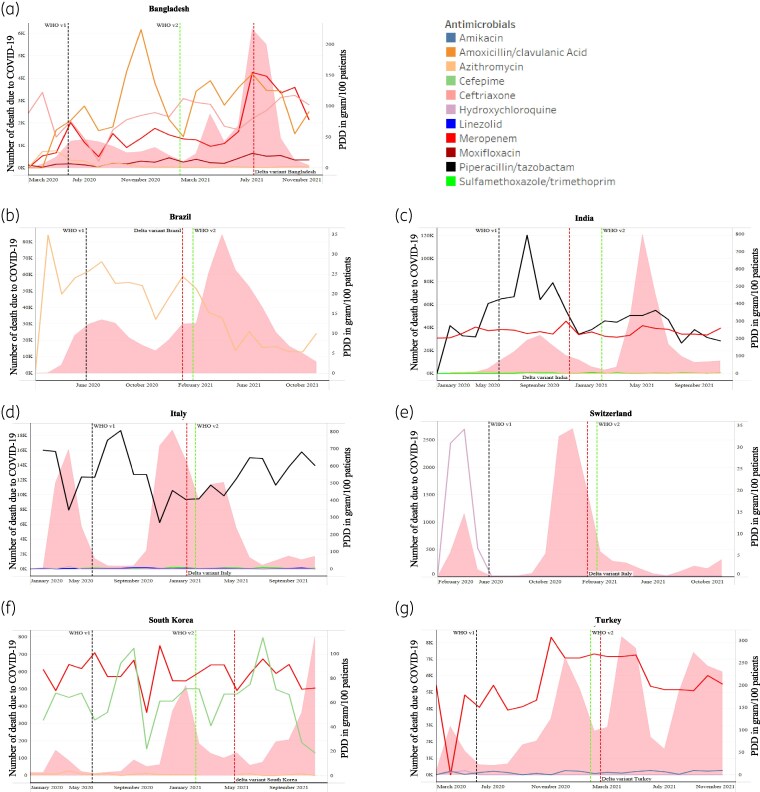
Results: Antimicrobials for which prescriptions significantly increased during the pandemic were as follows: meropenem in Bangladesh (95% CI: 1.94-4.07) with increased prescribed daily dose (PDD) (95% CI: 1.17-1.58) and Turkey (95% CI: 1.09-1.58), moxifloxacin in Bangladesh (95% CI: 4.11-11.87) with increased days of therapy (DOT) (95% CI: 1.14-2.56), piperacillin/tazobactam in Italy (95% CI: 1.07-1.48) with increased DOT (95% CI: 1.01-1.25) and PDD (95% CI: 1.05-1.21) and azithromycin in Bangladesh (95% CI: 3.36-21.77) and Brazil (95% CI: 2.33-8.42). ITSA showed a significant drop in azithromycin usage in India (95% CI: -8.38 to -3.49 g/100 patients) and South Korea (95% CI: -2.83 to -1.89 g/100 patients) after WHO guidelines v1 release and increased meropenem usage (95% CI: 93.40-126.48 g/100 patients) and moxifloxacin (95% CI: 5.40-13.98 g/100 patients) in Bangladesh and sulfamethoxazole/trimethoprim in India (95% CI: 0.92-9.32 g/100 patients) following the Delta variant emergence.
Conclusions: This study reinforces the importance of developing antimicrobial stewardship in the clinical settings during inter-pandemic periods.
© The Author(s) 2025. Published by Oxford University Press on behalf of British Society for Antimicrobial Chemotherapy.
Figures
References
-
- WHO . COVID-19 Public Health Emergency of International Concern (PHEIC) Global Research and Innovation Forum. https://www.who.int/publications/m/item/covid-19-public-health-emergency....
Grants and funding
LinkOut - more resources
Full Text Sources