

Heterogeneity of treatment effect of vilobelimab in COVID-19: a secondary analysis of a randomised controlled trial
- PMID: 38943192
- PMCID: PMC11214248
- DOI: 10.1186/s13054-024-05004-z
Heterogeneity of treatment effect of vilobelimab in COVID-19: a secondary analysis of a randomised controlled trial
Abstract
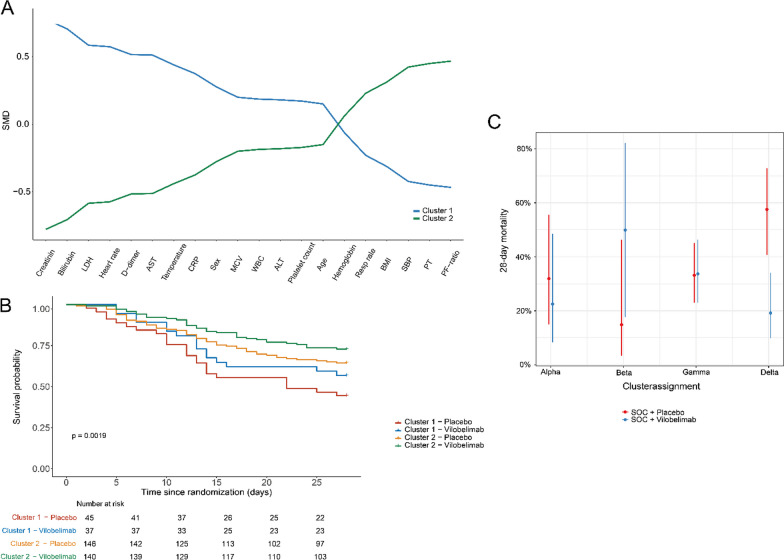
In a phase 3 trial (PANAMO, NCT04333420), vilobelimab, a complement 5a (C5a) inhibitor, reduced 28-day mortality in mechanically ventilated COVID-19 patients. This post hoc analysis of 368 patients aimed to explore treatment heterogeneity through unsupervised learning. All available clinical variables at baseline were used as input. Treatment heterogeneity was assessed using latent class analysis (LCA), Ward's hierarchical clustering (HC) and the adjudication to previously described clinical sepsis phenotypes. The primary outcome was 28-day mortality. For LCA, a 2-class latent model was deemed most suitable. In the LCA model, 82 (22%) patients were assigned to class 1 and 286 (78%) to class 2. Class 1 was defined by more severely ill patients with significantly higher mortality. In an adjusted logistic regression, no heterogeneity of treatment effect (HTE) between classes was observed (p = 0.998). For HC, no significant classes were found (p = 0.669). Using the previously described clinical sepsis subtypes, 41 patients (11%) were adjudicated subtype alpha (α), 17 (5%) beta (β), 112 (30%) delta (δ) and 198 (54%) gamma (γ). HTE was observed between clinical subtypes (p = 0.001) with improved 28-day mortality after treatment with vilobelimab for the δ subtype (OR = 0.17, 95% CI 0.07-0.40, p < 0.001). No signal for harm of treatment with vilobelimab was observed in any class or clinical subtype. Overall, treatment effect with vilobelimab was consistent across different classes and subtypes, except for the δ subtype, suggesting potential additional benefit for the most severely ill patients.
Keywords: COVID-19; Cluster analysis; Complement; Immunomodulation; Phenotype; Subtypes; Vilobelimab.
© 2024. The Author(s).
Conflict of interest statement
SR is an employee of Metronomia Clinical Research and a contracted statistical service provider for InflaRx. BPB is an employees of InflaRx and may hold shares and/or stock options in InflaRx. LDJB received consultancy fees from Scailyte, Santhera and Janssen en Janssen, and was on the advisory board of Sobi, Exvastat, Pfizer and Astra Zeneca, all paid to the institution. NCR is founder, active officer, and executive director of the board, and holds shares and stock options in InflaRx. APJV received consulting fees from InflaRx for advisory work, paid to the institution. The other authors have no competing interests.
Figures
References
-
- Vlaar APJ, Witzenrath M, van Paassen P, Heunks LMA, Mourvillier B, de Bruin S, et al. Anti-C5a antibody (vilobelimab) therapy for critically ill, invasively mechanically ventilated patients with COVID-19 (PANAMO): a multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Respir Med. 2022;10(12):1137–1146. doi: 10.1016/S2213-2600(22)00297-1. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
