

A Longitudinal Study of Ebola Sequelae in Liberia
- PMID: 30855742
- PMCID: PMC6478393
- DOI: 10.1056/NEJMoa1805435
A Longitudinal Study of Ebola Sequelae in Liberia
Abstract
Background: Multiple health problems have been reported in survivors of Ebola virus disease (EVD). Attribution of these problems to the disease without a control group for analysis is difficult.
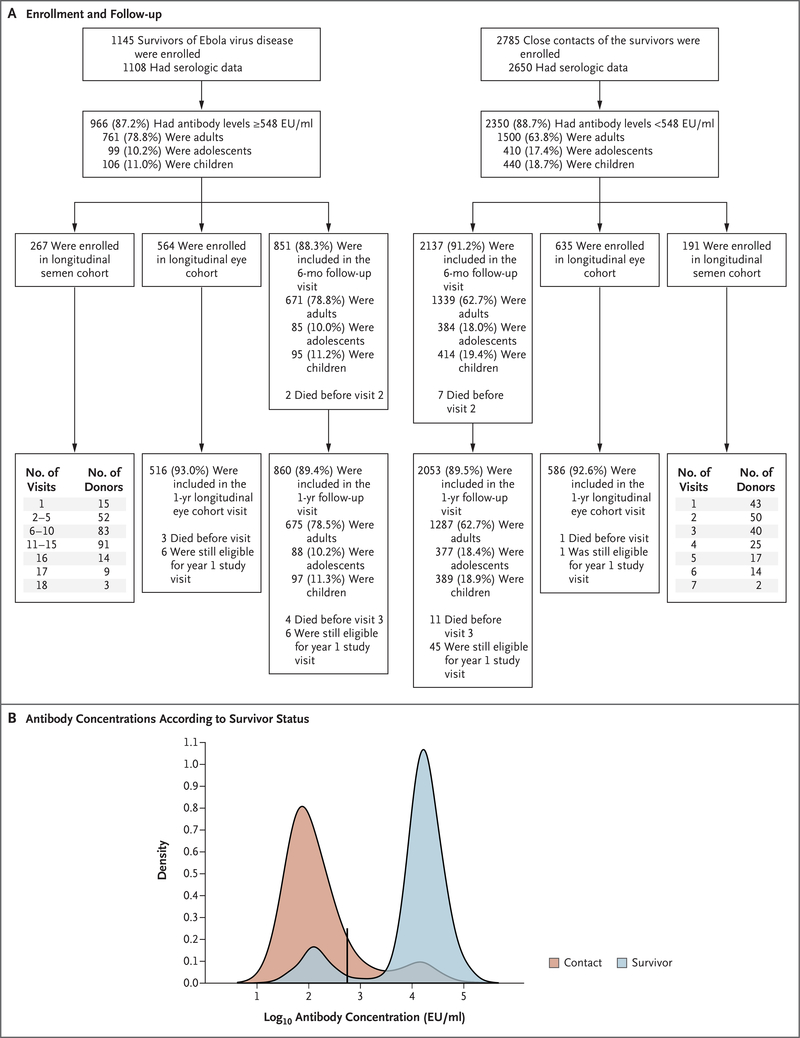
Methods: We enrolled a cohort of EVD survivors and their close contacts and prospectively collected data on symptoms, physical examination findings, and laboratory results. A subset of participants underwent ophthalmologic examinations. Persistence of Ebola virus (EBOV) RNA in semen samples from survivors was determined.
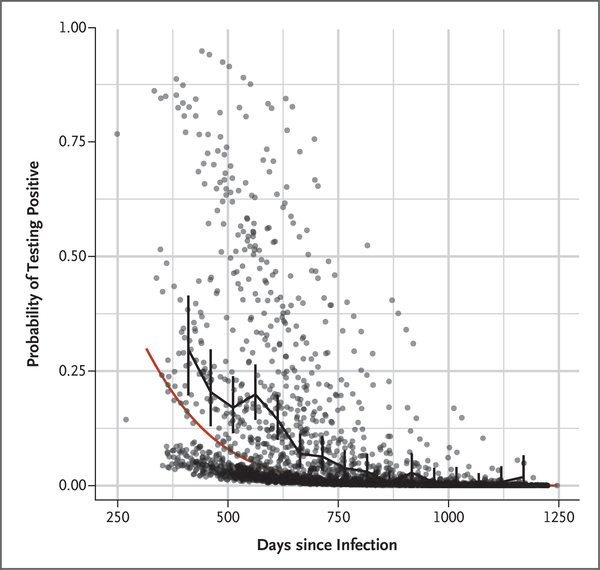
Results: A total of 966 EBOV antibody-positive survivors and 2350 antibody-negative close contacts (controls) were enrolled, and 90% of these participants were followed for 12 months. At enrollment (median time to baseline visit, 358 days after symptom onset), six symptoms were reported significantly more often among survivors than among controls: urinary frequency (14.7% vs. 3.4%), headache (47.6% vs. 35.6%), fatigue (18.4% vs. 6.3%), muscle pain (23.1% vs. 10.1%), memory loss (29.2% vs. 4.8%), and joint pain (47.5% vs. 17.5%). On examination, more survivors than controls had abnormal abdominal, chest, neurologic, and musculoskeletal findings and uveitis. Other than uveitis (prevalence at enrollment, 26.4% vs. 12.1%; at year 1, 33.3% vs. 15.4%), the prevalence of these conditions declined during follow-up in both groups. The incidence of most symptoms, neurologic findings, and uveitis was greater among survivors than among controls. EBOV RNA was detected in semen samples from 30% of the survivors tested, with a maximum time from illness to detection of 40 months.
Conclusions: A relatively high burden of symptoms was seen in all participants, but certain symptoms and examination findings were more common among survivors. With the exception of uveitis, these conditions declined in prevalence during follow-up in both groups. Viral RNA in semen persisted for a maximum of 40 months. (Funded by the National Institute of Allergy and Infectious Diseases and the National Eye Institute; PREVAIL III ClinicalTrials.gov number, NCT02431923.).
Copyright © 2019 Massachusetts Medical Society.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Ebola situation report. Geneva: World Health Organization, May 19, 2016. (https://www.who.int/csr/disease/ebola/situation-reports/archive/en/).
-
- Clark DV, Kibuuka H, Millard M, et al. Long-term sequelae after Ebola virus disease in Bundibugyo, Uganda: a retrospective cohort study. Lancet Infect Dis 2015; 15:905–12. - PubMed
-
- Etard JF, Sow MS, Leroy S, et al. Multidisciplinary assessment of post-Ebola sequelae in Guinea (Postebogui): an observational cohort study. Lancet Infect Dis 2017;17:545–52. - PubMed
-
- Kibadi K, Mupapa K, Kuvula K, et al. Late ophthalmologic manifestations in survivors of the 1995 Ebola virus epidemic in Kikwit, Democratic Republic of the Congo. J Infect Dis 1999;179:Suppl 1:S13–S14. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical