

World Health Organization Global Estimates and Regional Comparisons of the Burden of Foodborne Disease in 2010
- PMID: 26633896
- PMCID: PMC4668832
- DOI: 10.1371/journal.pmed.1001923
World Health Organization Global Estimates and Regional Comparisons of the Burden of Foodborne Disease in 2010
Abstract
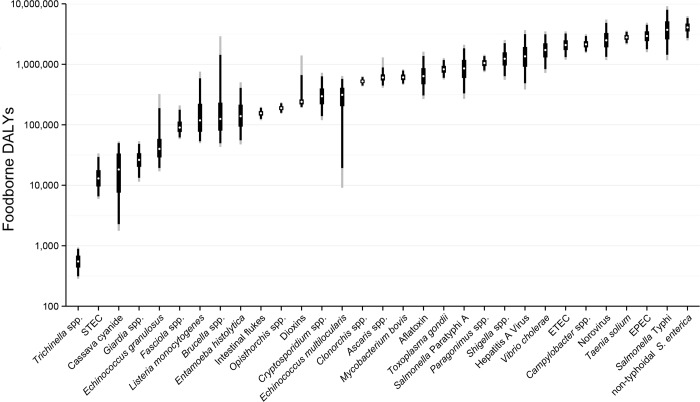
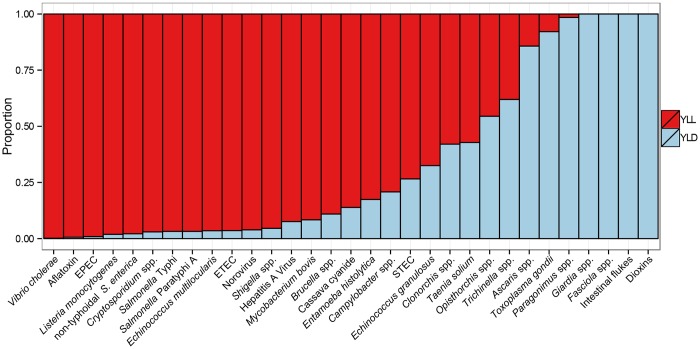
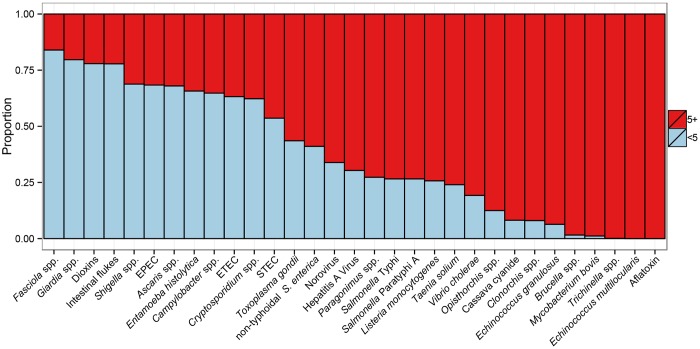
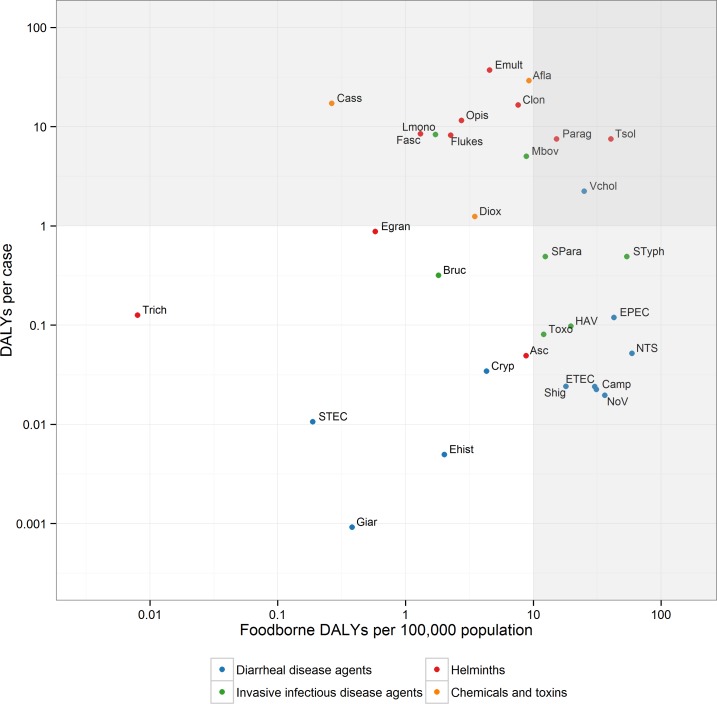
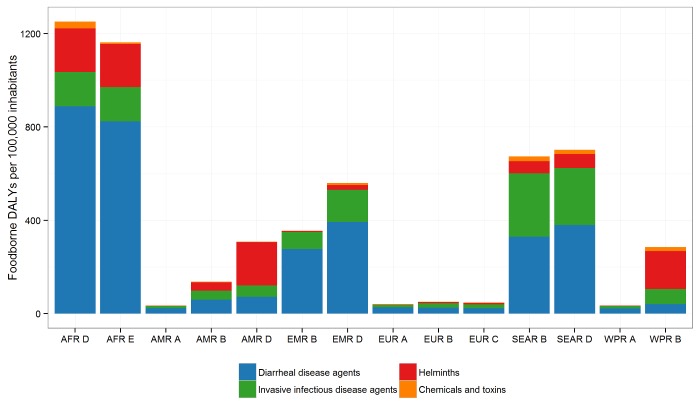
Illness and death from diseases caused by contaminated food are a constant threat to public health and a significant impediment to socio-economic development worldwide. To measure the global and regional burden of foodborne disease (FBD), the World Health Organization (WHO) established the Foodborne Disease Burden Epidemiology Reference Group (FERG), which here reports their first estimates of the incidence, mortality, and disease burden due to 31 foodborne hazards. We find that the global burden of FBD is comparable to those of the major infectious diseases, HIV/AIDS, malaria and tuberculosis. The most frequent causes of foodborne illness were diarrheal disease agents, particularly norovirus and Campylobacter spp. Diarrheal disease agents, especially non-typhoidal Salmonella enterica, were also responsible for the majority of deaths due to FBD. Other major causes of FBD deaths were Salmonella Typhi, Taenia solium and hepatitis A virus. The global burden of FBD caused by the 31 hazards in 2010 was 33 million Disability Adjusted Life Years (DALYs); children under five years old bore 40% of this burden. The 14 subregions, defined on the basis of child and adult mortality, had considerably different burdens of FBD, with the greatest falling on the subregions in Africa, followed by the subregions in South-East Asia and the Eastern Mediterranean D subregion. Some hazards, such as non-typhoidal S. enterica, were important causes of FBD in all regions of the world, whereas others, such as certain parasitic helminths, were highly localised. Thus, the burden of FBD is borne particularly by children under five years old-although they represent only 9% of the global population-and people living in low-income regions of the world. These estimates are conservative, i.e., underestimates rather than overestimates; further studies are needed to address the data gaps and limitations of the study. Nevertheless, all stakeholders can contribute to improvements in food safety throughout the food chain by incorporating these estimates into policy development at national and international levels.
Conflict of interest statement
AHH, MDK, PRT, HJG, TH, RJL, NP, FJA, DB, NdS, NG, NS, and BD serve as members of the World Health Organization advisory body—the Foodborne Disease Burden Epidemiology Reference Group—without remuneration. The authors declare no competing interests.
Figures
References
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–60. 10.1016/S0140-6736(12)61766-8 - DOI - PMC - PubMed
-
- World Health Organization. WHO consultation to develop a strategy to estimate the global burden of foodborne diseases Geneva, Switzerland: World Health Organization, 2006. http://www.who.int/foodsafety/publications/burden_sept06/en/
-
- FERG. World Health Organization Estimates of the Global Burden of Foodborne Disease. PLOS Collections. http://collections.plos.org/ferg-2015 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
