

Improving Assessment, Diagnosis, and Management of Urinary Incontinence and Lower Urinary Tract Symptoms on Acute and Rehabilitation Wards That Admit Adult Patients: Protocol for a Before-and-After Implementation Study
- PMID: 33538703
- PMCID: PMC7892286
- DOI: 10.2196/22902
Improving Assessment, Diagnosis, and Management of Urinary Incontinence and Lower Urinary Tract Symptoms on Acute and Rehabilitation Wards That Admit Adult Patients: Protocol for a Before-and-After Implementation Study
Abstract
Background: Urinary incontinence (UI) and lower urinary tract symptoms (LUTS) are commonly experienced by adult patients in hospitals (inpatients). Although peak bodies recommend that health services have systems for optimal UI and LUTS care, they are often not delivered. For example, results from the 2017 Australian National Stroke Audit Acute Services indicated that of the one-third of acute stroke inpatients with UI, only 18% received a management plan. In the 2018 Australian National Stroke Audit Rehabilitation Services, half of the 41% of patients with UI received a management plan. There is little reporting of effective inpatient interventions to systematically deliver optimal UI/LUTS care.
Objective: This study aims to determine whether our UI/LUTS practice-change package is feasible and effective for delivering optimal UI/LUTS care in an inpatient setting. The package includes our intervention that has been synthesized from the best-available evidence on UI/LUTS care and a theoretically informed implementation strategy targeting identified barriers and enablers. The package is targeted at clinicians working in the participating wards.
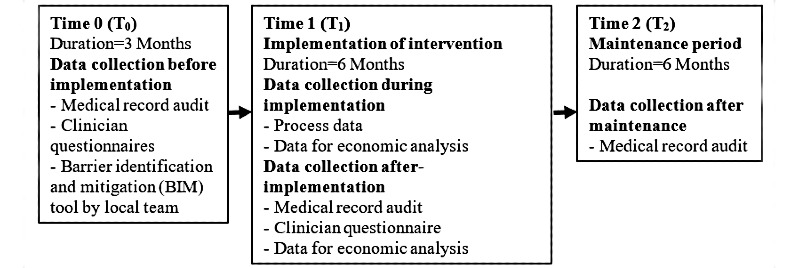
Methods: This is a pragmatic, real-world, before- and after-implementation study conducted at 12 hospitals (15 wards: 7/15, 47% metropolitan, 8/15, 53% regional) in Australia. Data will be collected at 3 time points: before implementation (T0), immediately after the 6-month implementation period (T1), and again after a 6-month maintenance period (T2). We will undertake medical record audits to determine any change in the proportion of inpatients receiving optimal UI/LUTS care, including assessment, diagnosis, and management plans. Potential economic implications (cost and consequences) for hospitals implementing our intervention will be determined.
Results: This study was approved by the Hunter New England Human Research Ethics Committee (HNEHREC Reference No. 18/10/17/4.02). Preimplementation data collection (T0) was completed in March 2020. As of November 2020, 87% (13/15) wards have completed implementation and are undertaking postimplementation data collection (T1).
Conclusions: Our practice-change package is designed to reduce the current inpatient UI/LUTS evidence-based practice gap, such as those identified through national stroke audits. This study has been designed to provide clinicians, managers, and policy makers with the evidence needed to assess the potential benefit of further wide-scale implementation of our practice-change package.
International registered report identifier (irrid): DERR1-10.2196/22902.
Keywords: inpatient; lower urinary tract symptoms; practice improvement; practice-gap; protocol; urinary incontinence.
©Dianne Lesley Marsden, Kerry Boyle, Louise-Anne Jordan, Judith Anne Dunne, Jodi Shipp, Fiona Minett, Amanda Styles, Jaclyn Birnie, Sally Ormond, Kim Parrey, Amanda Buzio, Sandra Lever, Michelle Paul, Kelvin Hill, Michael R P Pollack, John Wiggers, Christopher Oldmeadow, Dominique Ann-Michele Cadilhac, Jed Duff, The I-SCAMP Project Team. Originally published in JMIR Research Protocols (http://www.researchprotocols.org), 04.02.2021.
Conflict of interest statement
Conflicts of Interest: This project forms the basis of author KB’s PhD Candidature (University of Newcastle, NSW, Australia).
Figures
References
-
- Abrams P, Cardozo L, Wagg A, Wein A. editors. Incontinence 6th Edition. Tokyo: International Continence Society (ICS) & International Consultation on Urological Diseases (ICUD); 2017. p. 2017.
-
- Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, Van Kerrebroeck P, Victor A, Wein A, Standardisation Sub-Committee of the International Continence Society The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003 Jan;61(1):37–49. doi: 10.1016/s0090-4295(02)02243-4. - DOI - PubMed
-
- Condon M, Mannion E, Molloy DW, O'Caoimh R. Urinary and Faecal Incontinence: Point Prevalence and Predictors in a University Hospital. Int J Environ Res Public Health. 2019 Jan 11;16(2) doi: 10.3390/ijerph16020194. https://www.mdpi.com/resolver?pii=ijerph16020194 - DOI - PMC - PubMed
-
- Junqueira JB, Santos VLCDG. Urinary incontinence in hospital patients: prevalence and associated factors. Rev Lat Am Enfermagem. 2018 Jan 08;25:e2970. doi: 10.1590/1518-8345.2139.2970. https://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-1169201700... - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
