

DFV890: a new oral NLRP3 inhibitor-tested in an early phase 2a randomised clinical trial in patients with COVID-19 pneumonia and impaired respiratory function
- PMID: 36104613
- PMCID: PMC9473473
- DOI: 10.1007/s15010-022-01904-w
DFV890: a new oral NLRP3 inhibitor-tested in an early phase 2a randomised clinical trial in patients with COVID-19 pneumonia and impaired respiratory function
Abstract
Background: Coronavirus-associated acute respiratory distress syndrome (CARDS) has limited effective therapy to date. NLRP3 inflammasome activation induced by SARS-CoV-2 in COVID-19 contributes to cytokine storm.
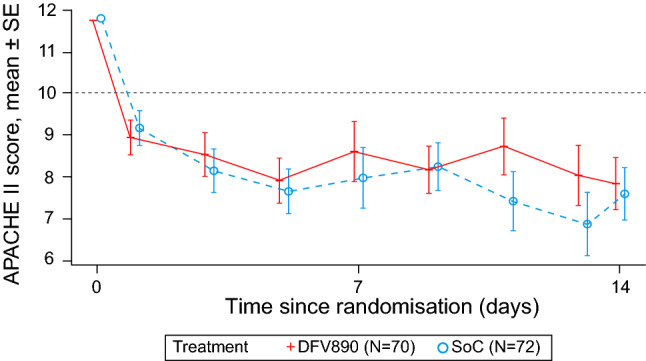
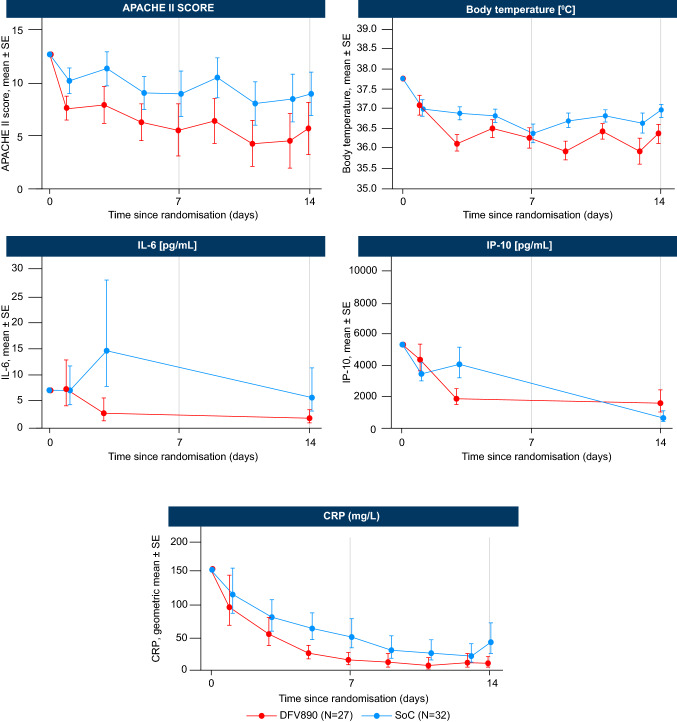
Methods: This randomised, multinational study enrolled hospitalised patients (18-80 years) with COVID-19-associated pneumonia and impaired respiratory function. Eligible patients were randomised (1:1) via Interactive Response Technology to DFV890 + standard-of-care (SoC) or SoC alone for 14 days. Primary endpoint was APACHE II score at Day 14 or on day-of-discharge (whichever-came-first) with worst-case imputation for death. Other key assessments included clinical status, CRP levels, SARS-CoV-2 detection, other inflammatory markers, in-hospital outcomes, and safety.
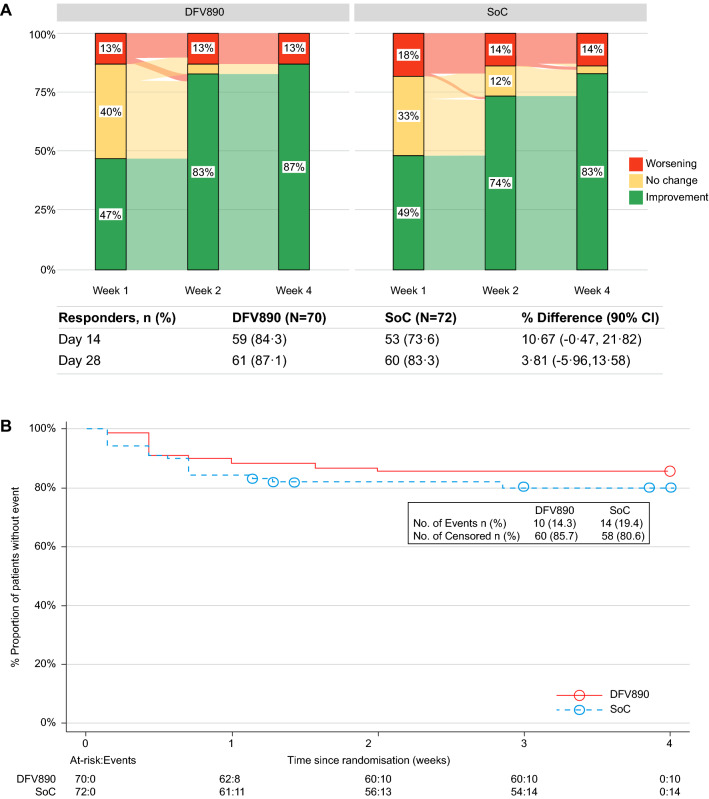
Findings: Between May 27, 2020 and December 24, 2020, 143 patients (31 clinical sites, 12 countries) were randomly assigned to DFV890 + SoC (n = 71) or SoC alone (n = 72). Primary endpoint to establish clinical efficacy of DFV890 vs. SoC, based on combined APACHE II score, was not met; LSM (SE), 8·7 (1.06) vs. 8·6 (1.05); p = 0.467. More patients treated with DFV890 vs. SoC showed ≥ 1-level improvement in clinical status (84.3% vs. 73.6% at Day 14), earlier clearance of SARS-CoV-2 (76.4% vs. 57.4% at Day 7), and mechanical ventilation-free survival (85.7% vs. 80.6% through Day 28), and there were fewer fatal events in DFV890 group (8.6% vs. 11.1% through Day 28). DFV890 was well tolerated with no unexpected safety signals.
Interpretation: DFV890 did not meet statistical significance for superiority vs. SoC in primary endpoint of combined APACHE II score at Day 14. However, early SARS-CoV-2 clearance, improved clinical status and in-hospital outcomes, and fewer fatal events occurred with DFV890 vs. SoC, and it may be considered as a protective therapy for CARDS.
Trial registration: ClinicalTrials.gov, NCT04382053.
Keywords: Coronavirus-associated acute respiratory distress syndrome; DFV890; NLRP3 inhibitors; Randomised controlled trial; SARS-CoV-2.
© 2022. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany.
Conflict of interest statement
Ildiko Madurka: none to declare. Alexander Vishnevsky: none to declare. Joan B. Soriano: received a grant from Novartis to conduct this trial via the Instituto de Investigación Hospital Universitario de la Princesa. Stephanus J. Gans: none to declare. Danilo Joel Salazar Ore: honorarium from Novartis for conducting this clinical trial at the Hospital Nacional Cayetano Heredia. Adrian Rendon: contract from Novartis as a PI in the Monterrry Investigation Center. Charlotte Suppli Ulrik: received fees for lectures, advisory board meetings, and presentations from AZ, GSK, BI, Chiesi, TEVA, Sanofi Genzyme, Novartis and Orion Pharma outside the submitted work. Sushma Bhatnagar: none to declare. Srikanth Krishnamurthy: received honoraria/research grants from AZ, BI, Sanofi, Novartis, Vicore Pharma, Sun Pharma, Dr. Reddys Lab, and Glenmark outside the submitted work. Kirsten Mc Harry: none declared. Tobias Welte: received research grant from German Ministry of Research and Education, German Ministry of Health; and fees for lectures/advisory board from AZ, Biontech, Roche, GSK, Novartis, Pfizer, Johnson & Johnson, Boehringer Ingelheim, and MSD; and advisory board honorarium from Novartis. Alberto Alfredo Fernandez: received honoraria for dissertations from AZ, Novartis, and BI. Guido Junge: employee and shareholder of Novartis. Beata Mehes: employee and shareholder of Novartis. Karin Meiser: employee of Novartis. Ewa Gatlik: Employee and shareholder of Novartis. Ulrike Sommer: employee and shareholder of Novartis. Ederlon Rezende: received research grants from Novartis and fees for lectures and presentations from Pfizer, Baxter, and MSD.
Figures

References
-
- World Health Organization. WHO coronavirus disease (COVID-19) dashboard. https://covid19.who.int/. Accessed 17 Jan 2022.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
