

Association between detection of HIV-1 DNA resistance mutations by a sensitive assay at initiation of antiretroviral therapy and virologic failure
- PMID: 20377404
- PMCID: PMC2856716
- DOI: 10.1086/652148
Association between detection of HIV-1 DNA resistance mutations by a sensitive assay at initiation of antiretroviral therapy and virologic failure
Abstract
Background: Antiretroviral therapy (ART) has become more available throughout the developing world during the past 5 years. The World Health Organization recommends nonnucleoside reverse-transcriptase inhibitor-based regimens as initial ART. However, their efficacy may be compromised by resistance mutations selected by single-dose nevirapine (sdNVP) used to prevent mother-to-child transmission of human immunodeficiency virus (HIV)-1. There is no simple and efficient method to detect such mutations at the initiation of ART.
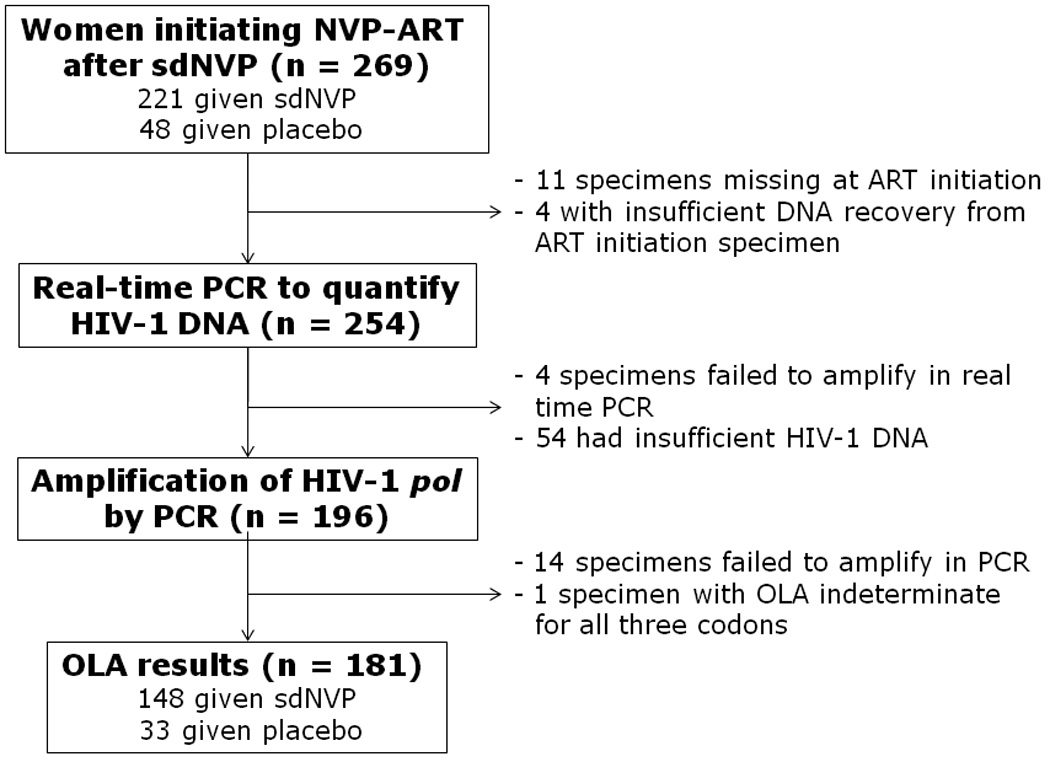
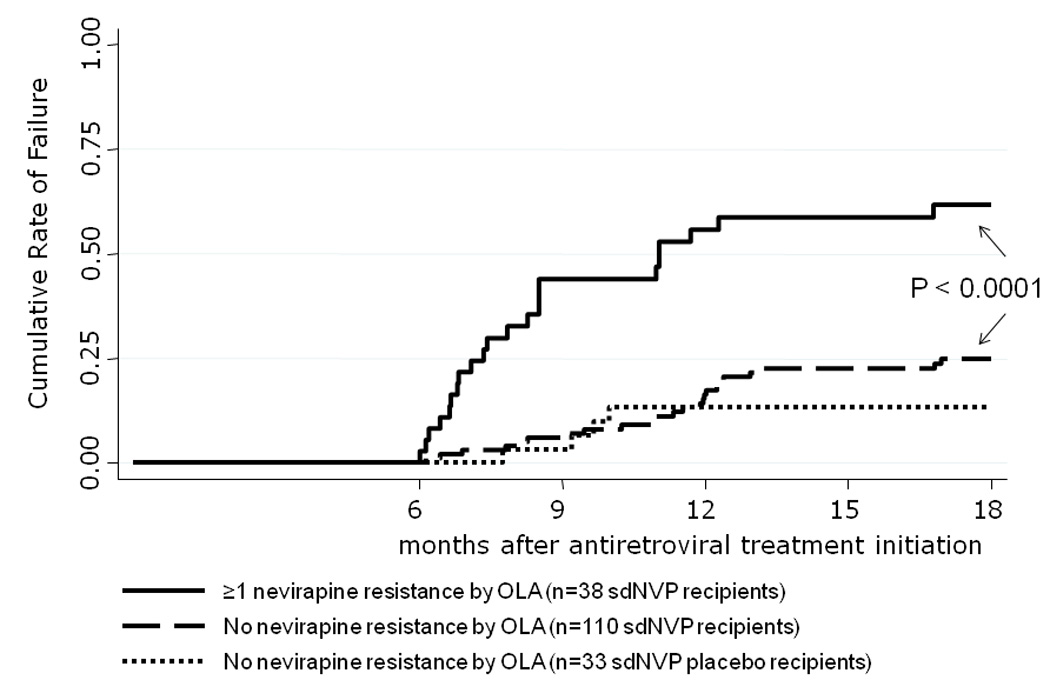
Methods: One hundred eighty-one women who were participating in a clinical trial to prevent mother-to-child transmission and who started NVP-ART after they had received sdNVP or a placebo were included in the study. One hundred copies of each patient's HIV-1 DNA were tested for NVP-resistance point-mutations (K103N, Y181C, and G190A) with a sensitive oligonucleotide ligation assay that was able to detect mutants even at low concentrations (> or = 5% of the viral population). Virologic failure was defined as confirmed plasma HIV-1 RNA >50 copies/mL after 6 to 18 months of NVP-ART.
Results: At initiation of NVP-ART, resistance mutations were identified in 38 (26%) of 148 participants given sdNVP (K103N in 19 [13%], Y181C in 8 [5%], G190A in 28 [19%], and > or = 2 mutations in 15 [10%]), at a median 9.3 months after receipt of sdNVP. The risk of virologic failure was 0.62 (95% confidence interval [CI], 0.46-0.77) in women with > or = 1% resistance mutation, compared with a risk of 0.25 (95% CI, 0.17-0.35) in those without detectable resistance mutations (P < .001). Failure was independently associated with resistance, an interval of <6 months between sdNVP and NVP-ART initiation, and a viral load higher than the median at NVP-ART initiation.
Conclusions: Access to simple and inexpensive assays to detect low concentrations of NVP-resistant HIV-1 DNA before the initiation of ART could help improve the outcome of first-line ART.
Conflict of interest statement
The authors have no other potential conflicts of interest to disclose.
Figures
References
-
- Jourdain G, Ngo-Giang-Huong N, Le Coeur S, et al. Intrapartum exposure to nevirapine and subsequent maternal responses to nevirapine-based antiretroviral therapy. N Engl J Med. 2004 Jul 15;351(3):229–240. - PubMed
-
- Lockman S, Shapiro RL, Smeaton LM, et al. Response to antiretroviral therapy after a single, peripartum dose of nevirapine. N Engl J Med. 2007 Jan 11;356(2):135–147. - PubMed
-
- Eshleman SH, Mracna M, Guay LA, et al. Selection and fading of resistance mutations in women and infants receiving nevirapine to prevent HIV-1 vertical transmission (HIVNET 012) Aids. 2001 Oct 19;15(15):1951–1957. - PubMed
-
- Weidle P, Stringer J, McConnell M, et al. Effectiveness of NNRTI-containing ART in Women Previously Exposed to a Single Dose of Nevirapine: A Multi-country Cohort Study; 15th Conference on Retroviruses and Opportunistic Infections.2008.
-
- Eshleman SH, Hoover DR, Chen S, et al. Nevirapine (NVP) resistance in women with HIV-1 subtype C, compared with subtypes A and D, after the administration of single-dose NVP. J Infect Dis. 2005 Jul 1;192(1):30–36. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
