Decoding the historical tale: COVID-19 impact on haematological malignancy patients-EPICOVIDEHA insights from 2020 to 2022
- PMID: 38533127
- PMCID: PMC10963230
- DOI: 10.1016/j.eclinm.2024.102553
Decoding the historical tale: COVID-19 impact on haematological malignancy patients-EPICOVIDEHA insights from 2020 to 2022
Abstract
Background: The COVID-19 pandemic heightened risks for individuals with hematological malignancies due to compromised immune systems, leading to more severe outcomes and increased mortality. While interventions like vaccines, targeted antivirals, and monoclonal antibodies have been effective for the general population, their benefits for these patients may not be as pronounced.
Methods: The EPICOVIDEHA registry (National Clinical Trials Identifier, NCT04733729) gathers COVID-19 data from hematological malignancy patients since the pandemic's start worldwide. It spans various global locations, allowing comprehensive analysis over the first three years (2020-2022).
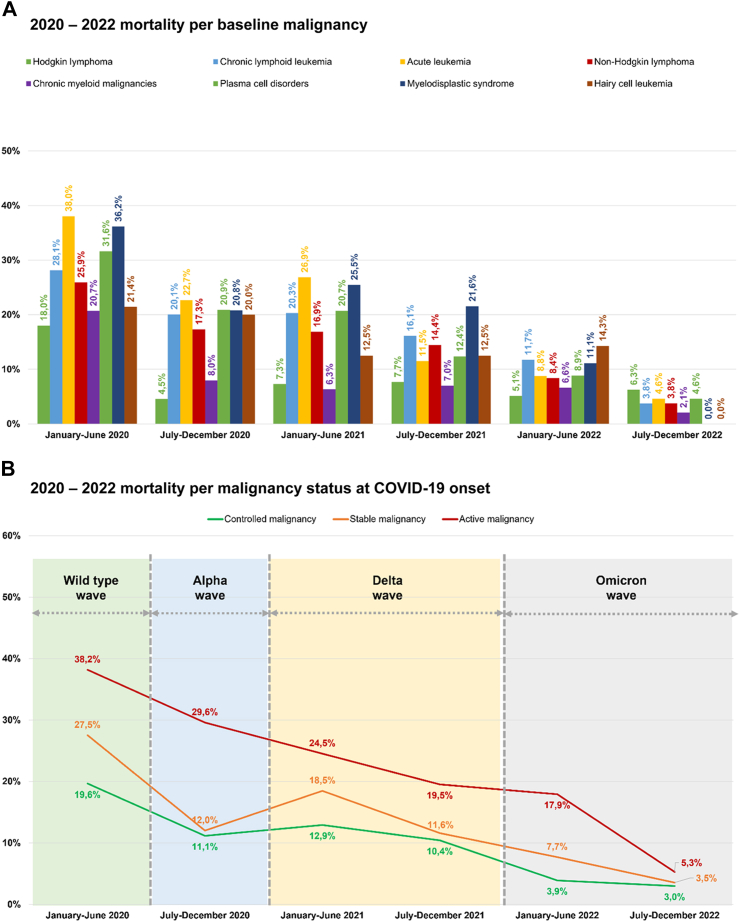
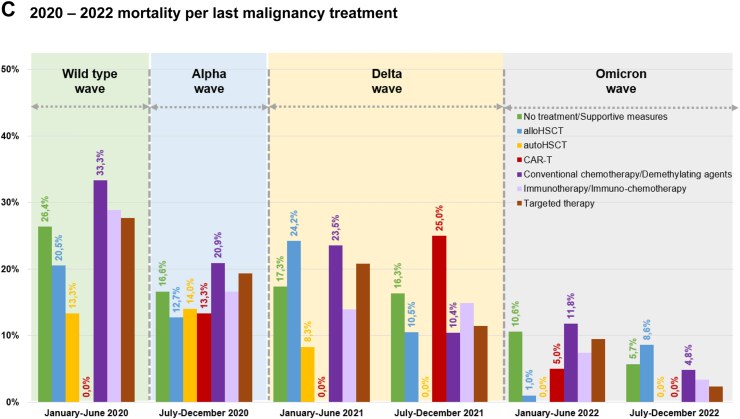
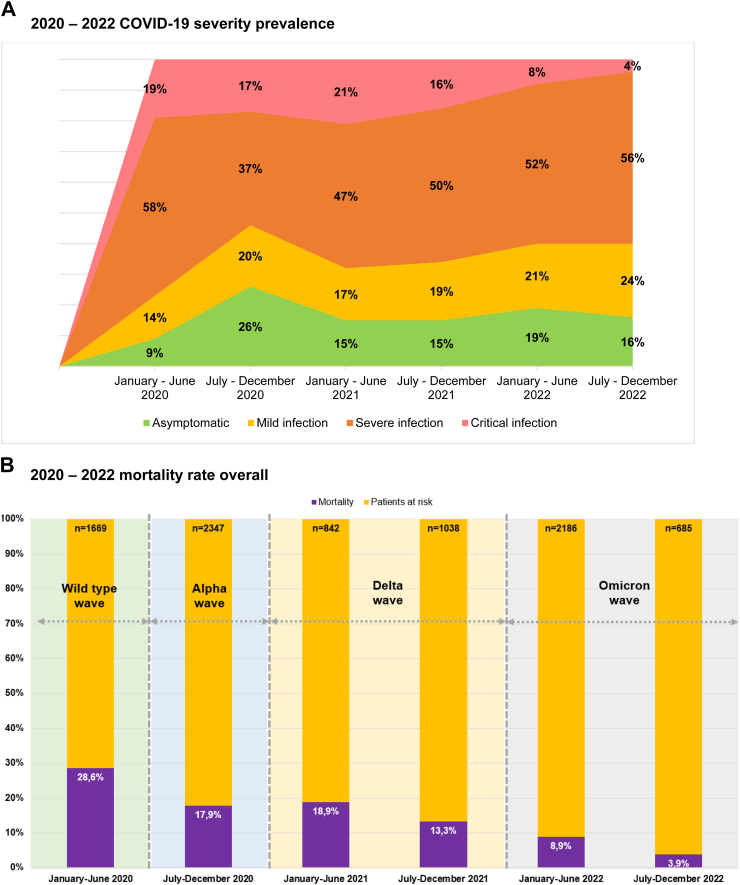
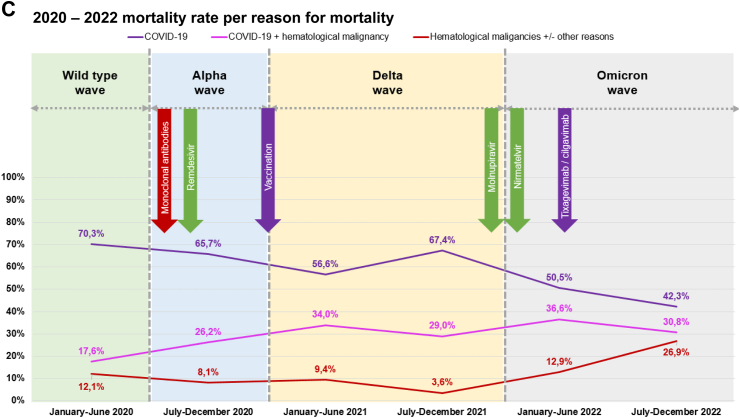
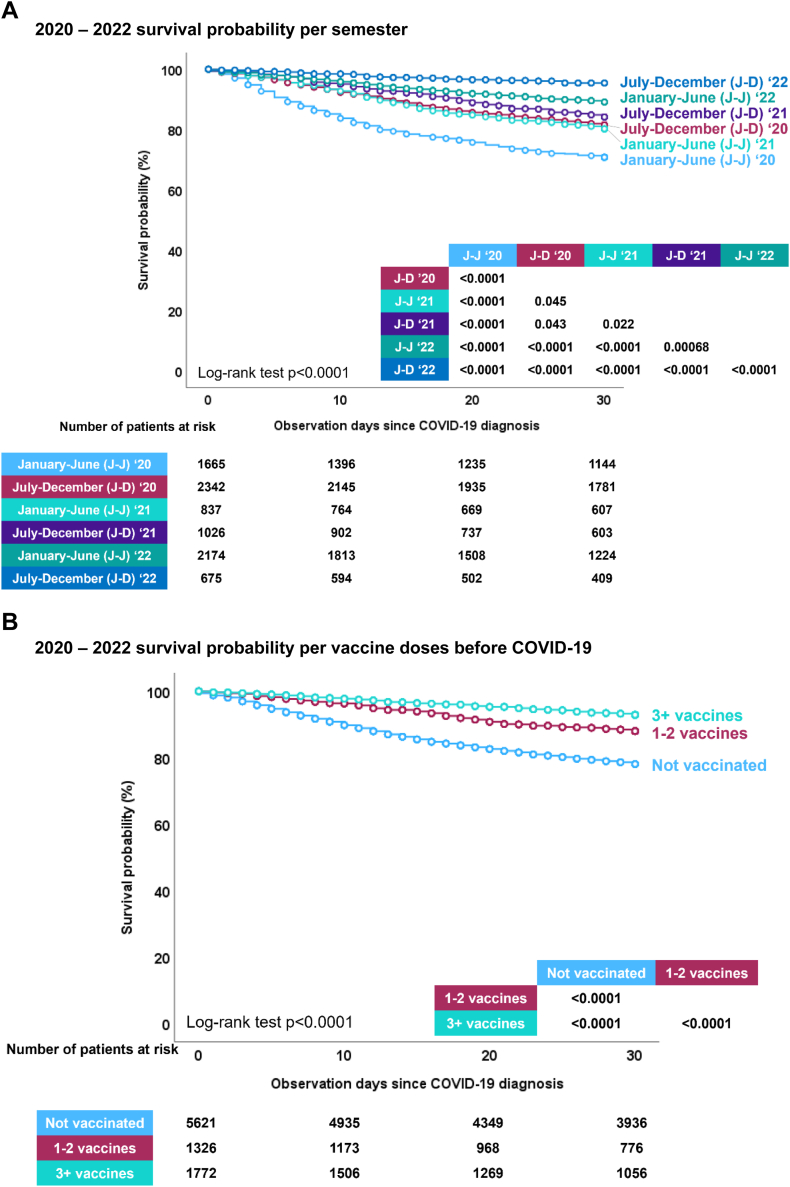
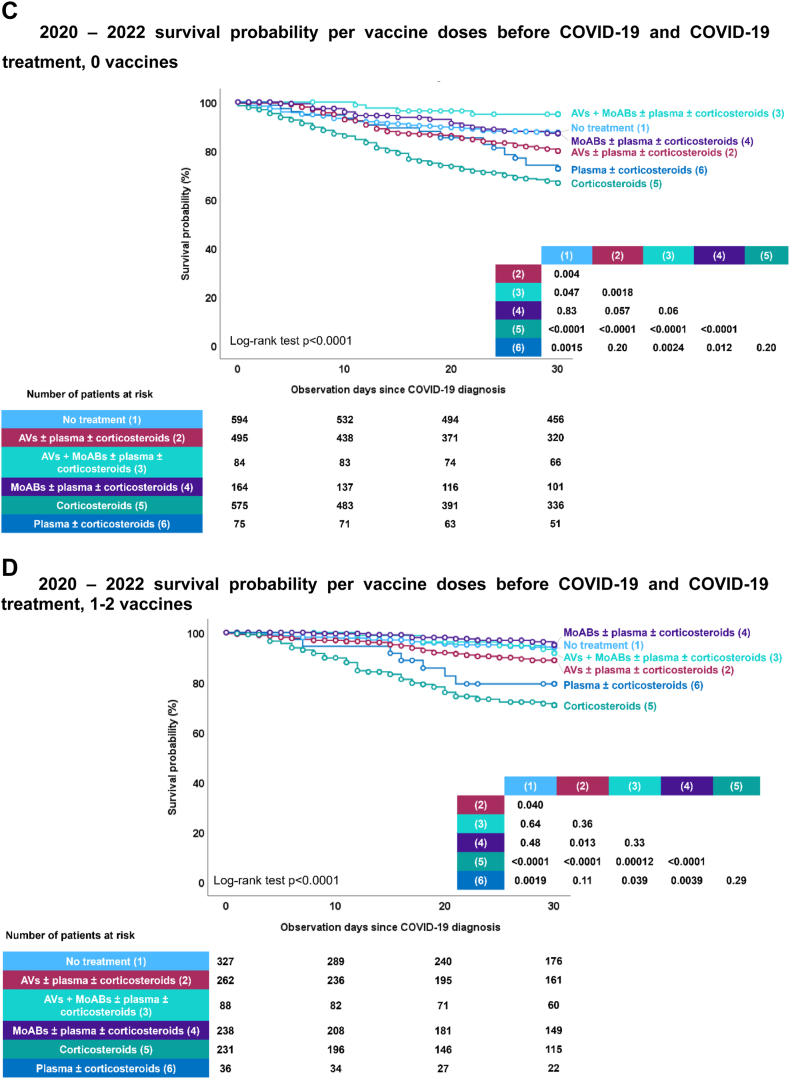
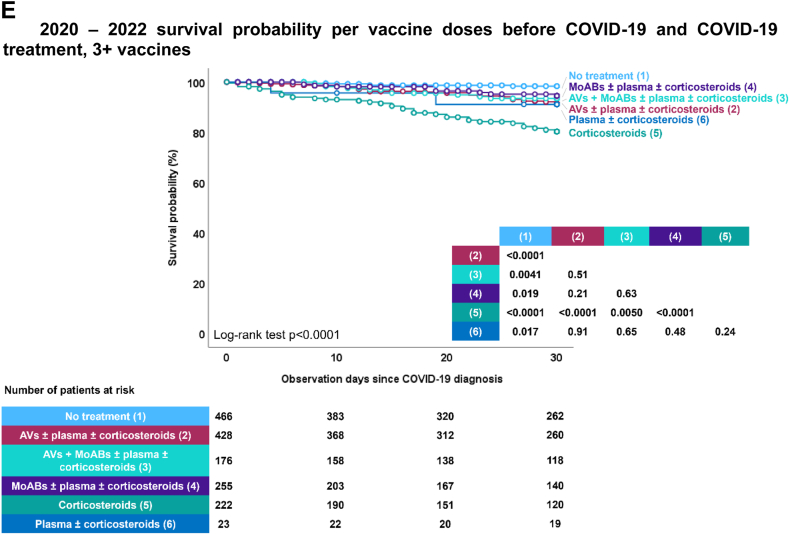
Findings: The EPICOVIDEHA registry collected data from January 2020 to December 2022, involving 8767 COVID-19 cases in hematological malignancy patients from 152 centers across 41 countries, with 42% being female. Over this period, there was a significant reduction in critical infections and an overall decrease in mortality from 29% to 4%. However, hospitalization, particularly in the ICU, remained associated with higher mortality rates. Factors contributing to increased mortality included age, multiple comorbidities, active malignancy at COVID-19 onset, pulmonary symptoms, and hospitalization. On the positive side, vaccination with one to two doses or three or more doses, as well as encountering COVID-19 in 2022, were associated with improved survival.
Interpretation: Patients with hematological malignancies still face elevated risks, despite reductions in critical infections and overall mortality rates over time. Hospitalization, especially in ICUs, remains a significant concern. The study underscores the importance of vaccination and the timing of COVID-19 exposure in 2022 for enhanced survival in this patient group. Ongoing monitoring and targeted interventions are essential to support this vulnerable population, emphasizing the critical role of timely diagnosis and prompt treatment in preventing severe COVID-19 cases.
Funding: Not applicable.
Keywords: COVID-19; Haematological malignancy; ICU; Immunosuppression; Vaccination.
© 2024 The Author(s).
Conflict of interest statement
JSG has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Gilead, Menarini, and Pfizer; and has participated on a Data Safety Monitoring Board or Advisory Board for Pfizer, outside of the submitted work. FI has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Novartis, AbbVie, Gilead; and has received support for attending meetings and/or travel from Novartis, AbbVie, Gilead, Astellas, Pfizer, Sanofi, BMS, Alexion, Astra-Zeneca, outside of the submitted work. MGdS has received grants or contracts from AstraZeneca, consulting fees from Roche, Janssen Cilag, Gilead, and Abbvie; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janssen; support for attending meetings and/or travel from Abbvie, Gilead, and Takeda; and participation on a Data Safety Monitoring Board or Advisory Board for Roche, Janssen Cilag, Lilly, Gilead, Takeda, and Abbvie, outside of the submitted work. ALG has received consulting fees from AstraZeneca; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Roche, Janssen, and Abbvie; and support for attending from meetings and/or travel from Astrazeneca, Janssen, and Beigene, outside of the submitted work. CGV has received grants or contracts from Ministerio de Sanidad y Consumo, Instituto de Salud Carlos III, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Gilead Science, MSD, Pfizer, Jannsen, Novartis, Basilea, GSK, Shionogi, AbbVie, Advanz Pharma, and a grant support from Gilead Science, Pfizer, GSK, MSD and Pharmamar, outside of the submitted work. MM has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Pfizer, GILEAD, MSD, and ViiV Healthcare; and support for attending meetings and/or travel from Pfizer, Pharmamar, Tillotts Pharma, outside of the submitted work. SKG has received grants or contracts from Else Kröner-Fresenius-Stiftung iPRIME Scholarship (2021_EKPK.10), UKE, Hamburg, outside of the submitted work. AV has received consulting fees from MSD and Takeda; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Gilead Pharma; and support for attending meetings and/or travel from Tillots, outside of the submitted work. TFA has received a pre-doctoral grant supported by the Ministerio de Sanidad y Consumo, Instituto de Salud Carlos III [RH RH042953], CM23/00277, outside of the submitted work. OAC has received grants or contracts from BMBF, Cidara, EU-DG RTD (101037867), F2G, Gilead, MedPace, MSD, Mundipharma, Octapharma, Pfizer, Scynexis; consulting fees from Abbvie, AiCuris, Biocon, Cidara, Gilead, IQVIA, Janssen, Matinas, MedPace, Menarini, Moderna, Molecular Partners, MSG-ERC, Noxxon, Octapharm, Pfizer, PSI, Scynexis, Seres; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Abbott, Abbvie, Al-Jazeera Pharmaceuticals/Hikma, Gilead, Grupo Biotoscana/United Medical/Knight, MedScape, MedUpdate, Merck/MSD, Noscendo, Pfizer, Shionogi, streamedup!; Payment for expert testimony from Cidara; a German patent (“Geschlossene Inkubationssysteme mit verbessertem Atemwegszugang für Untersuchungsvorrichtungen”, DE 10 2021 113 007.7), filed by the University of Cologne and listing Oliver A. Cornely as one of three inventors; Participation on a Data Safety Monitoring Board or Advisory Board from Boston Strategic Partners, Cidara, IQVIA, Janssen, MedPace, PSI, Pulmocide, Shionogi, The Prime Meridian Group; Stock or stock options from CoRe Consulting, EasyRadiology; and Other financial or non-financial interests from Wiley, outside of the submitted work. JM has received consulting fees from Takeda, F2G, and Mundipharma; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Takeda, F2G, and Mundipharma; and participation on a data safety monitoring board or advisory board from Takeda and Mundipharma, outside of the submitted work. JB has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janseen, Takeda and Pfizer and support for attending meetings and/or travel from Janssen and Pfizer, outside of the submitted work. ASO has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Pfizer, Gilead, MSD, and BioMeriuex, outside of the submitted work. CDR has received grants or contracts from Asociación Española Contra el Cáncer: Code Grant: CLJUN18010DERA (01/10/18–30/11/22), outside of the submitted work. NK has received propatient research grant: Third Party Donor Registry for personalized antiviral T-Cell immunotherapeutics, no. pp 20–34; SNSF: Epstein–Barr virus-specific T memory stem cell therapy, Projektförderung (Abt. I-III), no. 204944, SNSF: NCCR AntiResist, no. 180541; consulting fees from MSD Sharp & Dome, Pfizer, Gilead Sciences, and Takeda; patents planes, issued or pending for corss protective epitopes of Aspergillus fumigatus and Candida albicans; participation on a data safety mornitoing board or advisory board or Idorsia and Pulmocide; and Leadership or fiduciary role in other board, society, committee or advocacy groups, paid or unpaid for Fungal Infection Network of Switzerland (FUNGINOS), outside of the submitted work. RDB has been conference speaker to Novartis, Kite/Gilead, Pfizer, Abbie, and Incyte; has received travel accommodation from Kite/Gilead; and has participated in Scientific advisory board for Novartis, Kite/Gilead, Janssen, and BMS, outside of the submitted work. JAHR has received grants or contracts from BMS/Celgene, Janssen, Sanofi, and GSK; Consulting fees from Janssen, Roche, Abbvie, Gilead, BMS/Celgene, Amgen, Takeda, Rovi, AstraZeneca, Sandoz Novartis, Celltrion, EusaPharm, Sanofi, Beigene, and Lilly; and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janssen, Roche, Abbvie, Gilead, BMS/Celgene, Amgen, Takeda, AstraZeneca, Beigene, Lilly, and GSK, outside of the submitted work. LD has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Pfizer; and support for attending meetings and/or travel from Pfizer, outside of the submitted work. PK has received grants from German Federal Ministry of Research and Education (BMBF) B-FAST (Bundesweites Forschungsnetz Angewandte Surveillance und Testung) and NAPKON (Nationales Pandemie Kohorten Netz, German National Pandemic Cohort Network) of the Network University Medicine (NUM) and the State of North Rhine-Westphalia; consulting fees from Ambu GmbH, Gilead Sciences, Mundipharma Resarch Limited, Noxxon N.V., Pfizer Pharma; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Akademie für Infektionsmedizin e.V., Ambu GmbH, Astellas Pharma, BioRad Laboratories Inc., European Confederation of Medical Mycology, Gilead Sciences, GPR Academy Ruesselsheim, HELIOS Kliniken GmbH, Jazz Pharmaceuticals Germany GmbH, medupdate GmbH, MedMedia GmbH, MSD Sharp & Dohme GmbH, Pfizer Pharma GmbH, Scilink Comunicación Científica SC and University Hospital, LMU Munich; A German patent application (“Geschlossene Intubationssysteme mit verbessertem Atemwegszugang für Untersuchungsvorrichtungen”, official file number DE 10 2021 113 007.7) has been filed by the University of Cologne; Participation on a Data Safety Monitoring Board or Advisory Board from Ambu GmbH, Gilead Sciences, Pfizer Pharma, Mundipharma Resarch Limited, Noxxon N.V.; and Other financial or non-financial interests from Elsevier, Wiley, outside of the submitted work. PJ has received Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from GSK; Payment for expert testimony from Takeda; Support for attending meetings and/or travel from AstraZeneca, Novartis; and Participation on a Data Safety Monitoring Board or Advisory Board Takeda, BMS, outside of the submitted work. All authors had full access to the data and had final responsibility for the decision to submit for publication.
Figures