

A primary care-based, multicomponent lifestyle intervention for overweight adolescent females
- PMID: 22331335
- PMCID: PMC3289521
- DOI: 10.1542/peds.2011-0863
A primary care-based, multicomponent lifestyle intervention for overweight adolescent females
Abstract
Background and objective: Most clinic-based weight control treatments for youth have been designed for preadolescent children by using family-based care. However, as adolescents become more autonomous and less motivated by parental influence, this strategy may be less appropriate. This study evaluated a primary care-based, multicomponent lifestyle intervention specifically tailored for overweight adolescent females.
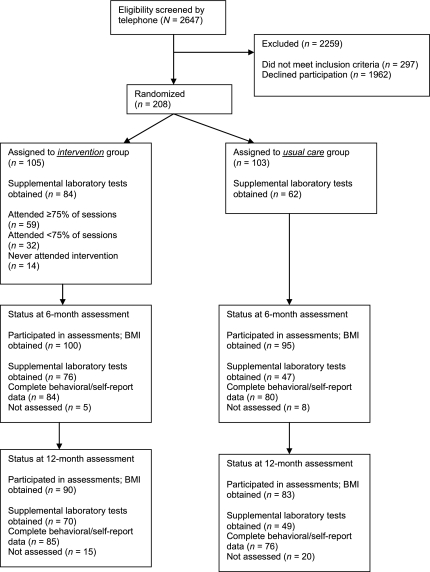
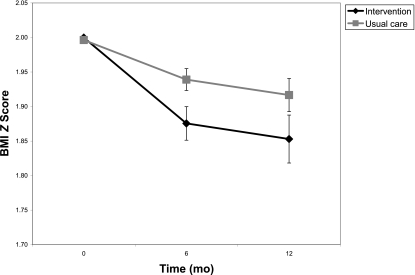
Methods: Adolescent girls (N = 208) 12 to 17 years of age (mean ± SD: 14.1 ± 1.4 years), with a mean ± SD BMI percentile of 97.09 ± 2.27, were assigned randomly to the intervention or usual care control group. The gender and developmentally tailored intervention included a focus on adoptable healthy lifestyle behaviors and was reinforced by ongoing feedback from the teen's primary care physician. Of those randomized, 195 (94%) completed the 6-month posttreatment assessment, and 173 (83%) completed the 12-month follow-up. The primary outcome was reduction in BMI z score.
Results: The decrease in BMI z score over time was significantly greater for intervention participants compared with usual care participants (-0.15 in BMI z score among intervention participants compared with -0.08 among usual care participants; P = .012). The 2 groups did not differ in secondary metabolic or psychosocial outcomes. Compared with usual care, intervention participants reported less reduction in frequency of family meals and less fast-food intake.
Conclusions: A 5-month, medium-intensity, primary care-based, multicomponent behavioral intervention was associated with significant and sustained decreases in BMI z scores among obese adolescent girls compared with those receiving usual care.
Trial registration: ClinicalTrials.gov NCT01068236.
Figures
Comment in
-
Pediatrics: tailoring weight-control programs to teenagers.Nat Rev Gastroenterol Hepatol. 2012 Mar 6;9(4):187. doi: 10.1038/nrgastro.2012.42. Nat Rev Gastroenterol Hepatol. 2012. PMID: 22392298 No abstract available.
References
-
- Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303(3):242–249 - PubMed
-
- Cook S, Weitzman M, Auinger P, Nguyen M, Dietz WH. Prevalence of a metabolic syndrome phenotype in adolescents: findings from the third National Health and Nutrition Examination Survey, 1988-1994. Arch Pediatr Adolesc Med. 2003;157(8):821–827 - PubMed
-
- Mossberg HO. 40-Year follow-up of overweight children. Lancet. 1989;2(8661):491–493 - PubMed
-
- Must A, Jacques PF, Dallal GE, Bajema CJ, Dietz WH. Long-term morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N Engl J Med. 1992;327(19):1350–1355 - PubMed
-
- Srinivasan SR, Bao W, Wattigney WA, Berenson GS. Adolescent overweight is associated with adult overweight and related multiple cardiovascular risk factors: the Bogalusa Heart Study. Metabolism. 1996;45(2):235–240 - PubMed
