

Phase 1/2 study of epacadostat in combination with ipilimumab in patients with unresectable or metastatic melanoma
- PMID: 30894212
- PMCID: PMC6425606
- DOI: 10.1186/s40425-019-0562-8
Phase 1/2 study of epacadostat in combination with ipilimumab in patients with unresectable or metastatic melanoma
Abstract
Background: Epacadostat is a potent inhibitor of the immunosuppressive indoleamine 2,3-dioxygenase 1 (IDO1) enzyme. We present phase 1 results from a phase 1/2 clinical study of epacadostat in combination with ipilimumab, an anti-cytotoxic T-lymphocyte-associated protein 4 antibody, in advanced melanoma (NCT01604889).
Methods: Only the phase 1, open-label portion of the study was conducted, per the sponsor's decision to terminate the study early based on the changing melanoma treatment landscape favoring exploration of programmed cell death protein 1 (PD-1)/PD-ligand 1 inhibitor-based combination strategies. Such decision was not related to the safety of epacadostat plus ipilimumab. Patients received oral epacadostat (25, 50, 100, or 300 mg twice daily [BID]; 75 mg daily [50 mg AM, 25 mg PM]; or 50 mg BID intermittent [2 weeks on/1 week off]) plus intravenous ipilimumab 3 mg/kg every 3 weeks.
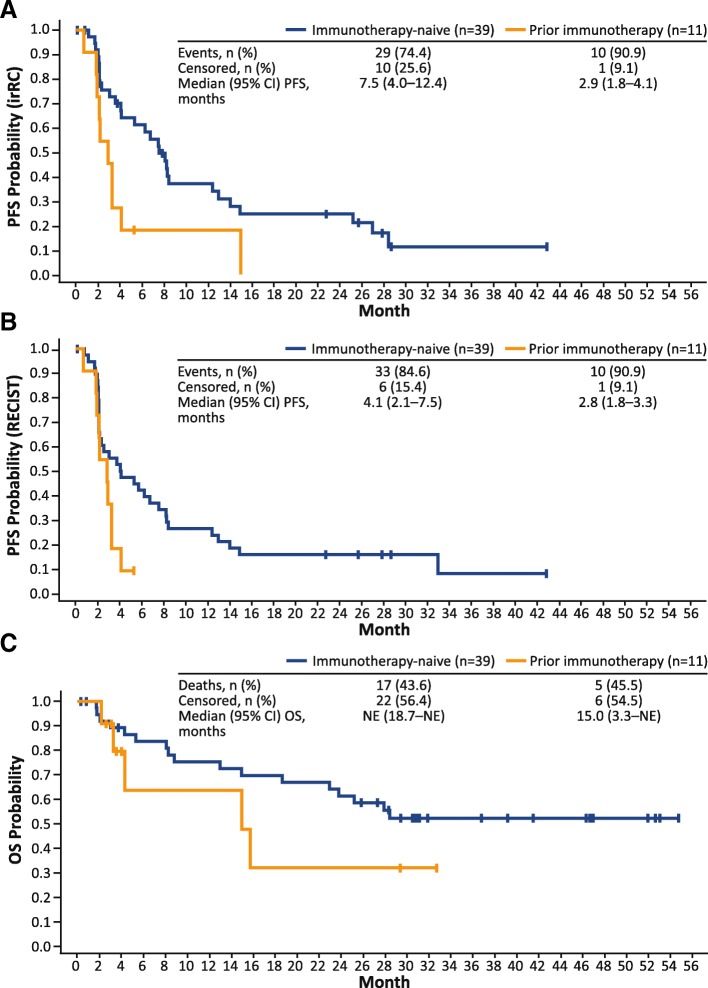
Results: Fifty patients received ≥1 dose of epacadostat. As of January 20, 2017, 2 patients completed treatment and 48 discontinued, primarily because of adverse events (AEs) and disease progression (n = 20 each). Dose-limiting toxicities occurred in 11 patients (n = 1 each with epacadostat 25 mg BID, 50 mg BID intermittent, 75 mg daily; n = 4 each with epacadostat 50 mg BID, 300 mg BID). The most common immune-related treatment-emergent AEs included rash (50%), alanine aminotransferase elevation (28%), pruritus (28%), aspartate aminotransferase elevation (24%), and hypothyroidism (10%). Among immunotherapy-naive patients (n = 39), the objective response rate was 26% by immune-related response criteria and 23% by Response Evaluation Criteria in Solid Tumors version 1.1. No objective response was seen in the 11 patients who received prior immunotherapy. Epacadostat exposure was dose proportional, with clinically significant IDO1 inhibition at doses ≥25 mg BID.
Conclusions: When combined with ipilimumab, epacadostat ≤50 mg BID demonstrated clinical and pharmacologic activity and was generally well tolerated in patients with advanced melanoma.
Trial registration: ClinicalTrials.gov identifier, NCT01604889 . Registration date, May 9, 2012, retrospectively registered.
Keywords: Epacadostat; IDO1; Immune checkpoint inhibition; Ipilimumab; Melanoma.
Conflict of interest statement
Ethics approval and consent to participate
This report was conducted in accordance with the provisions of the Declaration of Helsinki, as described in the International Council for Harmonisation Guidelines for Good Clinical Practice, and was approved by the institutional review board at each participating institution. All patients provided informed consent before initiation of treatment.
Consent for publication
Not applicable.
Competing interests
GTG served as a consultant for Array BioPharma, Genentech, Novartis, Incyte Corporation, Newlink Genetics, Jounce, and Bristol-Myers Squibb; and served on a speakers bureau for Genentech. OH served consulting or advisory roles with Amgen, Novartis, Roche, Bristol-Myers Squibb, and Merck; served on speakers bureaus for Bristol-Myers Squibb, Genentech, Novartis, and Amgen; and received research funding from AstraZeneca, Bristol-Myers Squibb, Celldex, Genentech, Immunocore, Incyte, Merck, Merck Serono, MedImmune, Novartis, Pfizer, Rinat, and Roche. JL served as an advisory board consultant for Bristol-Myers Squibb. AJO served consulting or advisory roles with Merck, Takeda, Bristol-Myers Squibb, and G1 Therapeutics; received research funding from Takeda, Immunocore, EMD Serono, Amgen, Incyte, Kyowa Hakko Kirin, Lilly, Advaxis, Mirati Therapeutics, Ignyta, Novartis, Pfizer, Bristol-Myers Squibb, and Kura; and received travel/accommodation expenses from Takeda. TCM served consulting or advisory roles with Novartis, Bristol-Myers Squibb, Merck, and Incyte; and received research funding from Merck, Incyte, Bristol-Myers Squibb, and Roche. TFG has received consultancy fees from Merck, Roche-Genentech, AbbVie, Bayer, Jounce, Aduro, Fog Pharma, Adaptimmune, FivePrime, and Sanofi; has received research support from Roche-Genentech, Bristol-Myers Squibb, Merck, Incyte, Seattle Genetics, Celldex, Ono, Evelo, Bayer, and Aduro; has intellectual property/licensing agreements with Aduro, Evelo, and Bristol-Myers Squibb; and is a cofounder/shareholder with Jounce. BC has nothing to disclose. BAH received research funding from Merck, OncoMed Pharmaceuticals, MedPacto Inc., GlaxoSmithKline, AstraZeneca, D3 A*STAR, and Tempest; served consulting or advisory roles for G1 Therapeutics and FujiFilm Pharmaceuticals; and served on speakers bureaus for CE Concepts and Merck. YZ was an employee and stockholder of Incyte Corporation at the time of data analysis. RCN, JM, and LL are employees and stockholders of Incyte Corporation. JSW owns equity in Biond, Altor, and CytomX; is named on patents for Biodesix (PD-1 biomarker) and Moffitt (CTLA-4 biomarker; neither of which were used in the current work); and has received consulting fees for advisory boards for Bristol-Myers Squibb, GlaxoSmithKline, Merck, Novartis, Incyte Corporation, Genentech, AstraZeneca, Celldex, Sellas, CytomX, EMD Serono, and Pfizer.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbe C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711–723. doi: 10.1056/NEJMoa1003466. - DOI - PMC - PubMed
-
- YERVOY® (ipilimumab). Full prescribing information, Bristol-Myers Squibb Company. Princeton, NJ; 2017.
-
- Hodi FS, Chesney J, Pavlick AC, Robert C, Grossmann KF, McDermott DF, Linette GP, Meyer N, Giguere JK, Agarwala SS, Shaheen M, Ernstoff MS, Minor DR, Salama AK, Taylor MH, Ott PA, Horak C, Gagnier P, Jiang J, Wolchok JD, Postow MA. Combined nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomised, controlled, phase 2 trial. Lancet Oncol. 2016;17:1558–1568. doi: 10.1016/S1470-2045(16)30366-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials