

Effectiveness of Task-Shifted Trauma-Focused Cognitive Behavioral Therapy for Children Who Experienced Parental Death and Posttraumatic Stress in Kenya and Tanzania: A Randomized Clinical Trial
- PMID: 31968059
- PMCID: PMC6990668
- DOI: 10.1001/jamapsychiatry.2019.4475
Effectiveness of Task-Shifted Trauma-Focused Cognitive Behavioral Therapy for Children Who Experienced Parental Death and Posttraumatic Stress in Kenya and Tanzania: A Randomized Clinical Trial
Abstract
Importance: Approximately 140 million children worldwide have experienced the death of one or both parents. These children, mostly in low- and middle-income countries, have higher rates of mental health problems than those who have not experienced parental death. Cognitive behavioral therapy (CBT) may improve the well-being of these children, but to our knowledge there have been no randomized clinical trials specifically focused on this population.
Objectives: To test the effectiveness of trauma-focused CBT (TF-CBT) for improving posttraumatic stress (PTS) in children in Kenya and Tanzania who have experienced parental death, to test the effects of TF-CBT on other mental health symptoms, and to examine the feasibility of task-shifting with greater reliance on experienced, local lay counselors as trainers and supervisors.
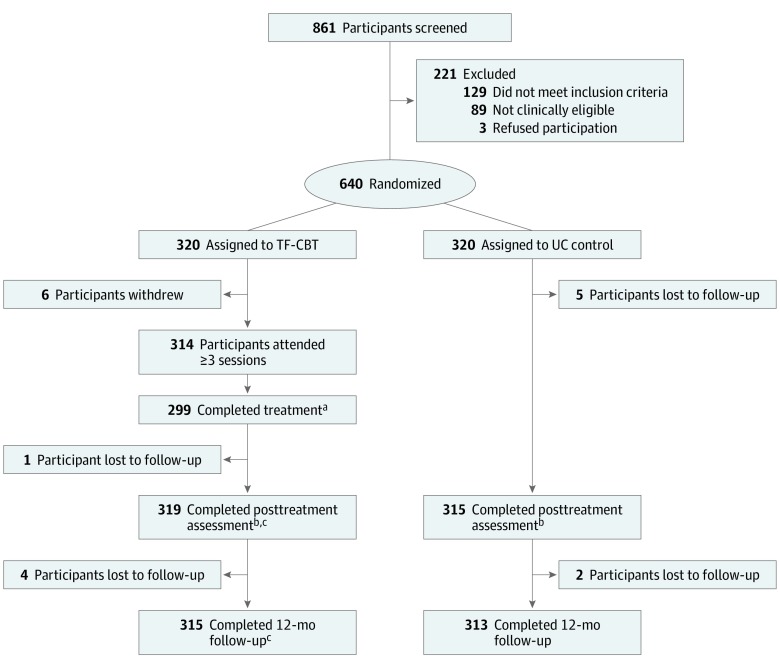
Design, setting, and participants: A randomized clinical trial conducted in urban and rural areas of Tanzania and Kenya compared TF-CBT and usual care (UC) for 640 children aged 7 to 13 years who were recruited from February 13, 2013, to July 24, 2015. All children had experienced the death of one or both parents and had elevated PTS and/or prolonged grief. Interviewers were masked to study condition. Participants were followed up for 12 months after the randomized clinical trial. Statistical analysis was performed from February 3, 2017, to August 26, 2019. All analyses were on an intent-to-treat basis.
Interventions: In the intervention condition, 320 children received 12 weeks of group TF-CBT delivered by lay counselors who were supervised weekly. In the UC condition, 320 children received community services typically offered to this population.
Main outcomes and measures: The primary outcome was PTS, evaluated using a continuous, standardized measure. Other mental health symptoms and child-guardian relationship were also measured.
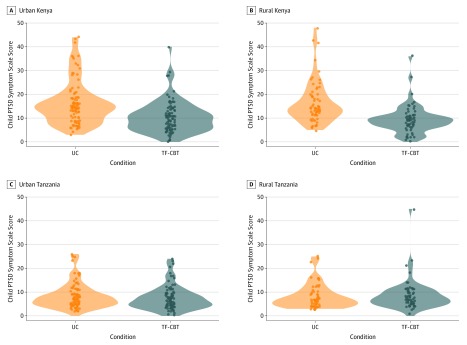
Results: A total of 640 children (320 girls and 320 boys; mean [SD] age, 10.6 [1.6] years) were included in the study. Trauma-focused CBT was more effective than UC for PTS in 3 of 4 sites after treatment (end of 3-month randomized clinical trial): rural Kenya (Cohen d = 1.04 [95% CI, 0.72-1.36]), urban Kenya (Cohen d = 0.56 [95% CI, 0.29-0.83]), and urban Tanzania (Cohen d = 0.45 [95% CI, 0.10-0.80]). At 12-month follow-up, TF-CBT remained more effective than UC in both rural (Cohen d = 0.86 [95% CI, 0.64-1.07]) and urban (Cohen d = 0.99 [95% CI, 0.75-1.23]) Kenya. At 12-month follow-up in Tanzania, children who received TF-CBT and UC had comparable rates of improvement (rural Tanzania, Cohen d = 0.09 [95% CI, -0.08 to 0.26]; urban Tanzania, Cohen d = 0.11 [95% CI, -0.09 to 0.31]). A similar pattern was seen for secondary outcomes, with stronger effects observed in Kenya, where children experienced greater stress and adversity (eg, more food scarcity, poorer guardian health, and greater exposure to traumatic events).
Conclusions and relevance: This study found that TF-CBT was more effective than UC in reducing PTS among children who experienced parental death in 3 of 4 sites in Kenya and Tanzania. At 12-month follow-up, TF-CBT was more effective in reducing PTS only among children in rural and urban Kenya.
Trial registration: ClinicalTrials.gov identifier: NCT01822366.
Conflict of interest statement
Figures
Comment in
-
Policy Makers' Tough Choices for Psychological Interventions in Global Mental Health: Learning From Multisite Studies.JAMA Psychiatry. 2020 May 1;77(5):452-454. doi: 10.1001/jamapsychiatry.2019.4267. JAMA Psychiatry. 2020. PMID: 31968064 Free PMC article. No abstract available.
References
-
- UNICEF The state of the world’s children 2016: a fair chance for every child. https://www.unicef.org/publications/files/UNICEF_SOWC_2016.pdf. Published June 2016. Accessed January 7, 2019.
-
- UNICEF Orphans. https://www.unicef.org/media/media_45279.html. Updated June 16, 2017. Accessed June 12, 2019.
-
- Urassa M, Boerma JT, Ng’weshemi JZL, Isingo R, Schapink D, Kumogola Y. . Orphanhood, child fostering and the AIDS epidemic in rural Tanzania: project to support AIDS control in Mwanza Region. Health Transit Rev. 1997;7(suppl 2):141-153.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
