

Randomised trial of intravenous thiamine and/or magnesium sulphate administration on erythrocyte transketolase activity, lactate concentrations and alcohol withdrawal scores
- PMID: 35484175
- PMCID: PMC9051209
- DOI: 10.1038/s41598-022-10970-x
Randomised trial of intravenous thiamine and/or magnesium sulphate administration on erythrocyte transketolase activity, lactate concentrations and alcohol withdrawal scores
Abstract
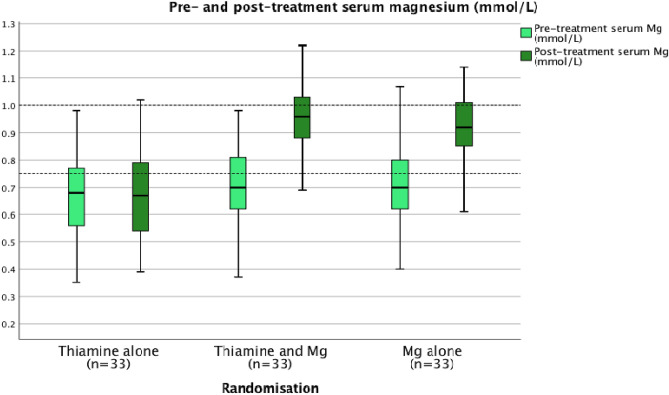
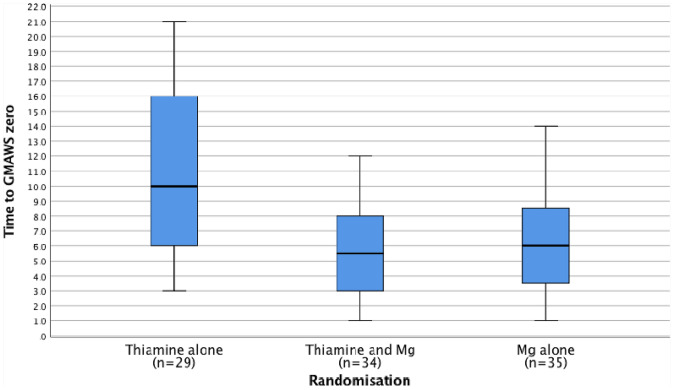
Alcohol withdrawal syndrome (AWS) occurs in 2% of patients admitted to U.K. hospitals. Routine treatment includes thiamine and benzodiazepines. Laboratory studies indicate that thiamine requires magnesium for optimal activity, however this has not translated into clinical practice. Patients experiencing AWS were randomized to three groups: (group 1) thiamine, (group 2) thiamine plus MgSO4 or (group 3) MgSO4. Pre- and 2-h post-treatment blood samples were taken. AWS severity was recorded using the Glasgow Modified Alcohol Withdrawal Score (GMAWS). The primary outcome measure was 15% change in erythrocyte transketolase activity (ETKA) in group 3. Secondary outcome measures were change in plasma lactate concentrations and time to GMAWS = 0. 127 patients were recruited, 115 patients were included in the intention-to-treat analysis. Pre-treatment, the majority of patients had normal or high erythrocyte thiamine diphosphate (TDP) concentrations (≥ 275-675/> 675 ng/gHb respectively) (99%), low serum magnesium concentrations (< 0.75 mmol/L) (59%), and high plasma lactate concentrations (> 2 mmol/L) (67%). Basal ETKA did not change significantly in groups 1, 2 or 3. Magnesium deficient patients (< 0.75 mmol/L) demonstrated less correlation between pre-treatment basal ETKA and TDP concentrations than normomagnesemic patients (R2 = 0.053 and R2 = 0.236). Median plasma lactate concentrations normalized (≤ 2.0 mmol/L) across all three groups (p < 0.001 for all groups), but not among magnesium deficient patients in group 1 (n = 22). The median time to achieve GMAWS = 0 for groups 1, 2 and 3 was 10, 5.5 and 6 h respectively (p < 0.001). No significant difference was found between groups for the primary endpoint of change in ETKA. Co-administration of thiamine and magnesium resulted in more consistent normalization of plasma lactate concentrations and reduced duration to achieve initial resolution of AWS symptoms.ClinicalTrials.gov: NCT03466528.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures








References
-
- WHO . Global Status Report on Alcohol and Health. World Health Organization; 2018.
-
- Maguire D, Talwar D, Burns A, Catchpole A, Stefanowicz F, Robson G, et al. A prospective evaluation of thiamine and magnesium status in relation to clinicopathological characteristics and 1-year mortality in patients with alcohol withdrawal syndrome. J. Transl. Med. 2019;17(1):384. doi: 10.1186/s12967-019-02141-w. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
