

A pragmatic clinical trial of cascade testing for familial hypercholesterolemia
- PMID: 36173399
- PMCID: PMC9944844
- DOI: 10.1016/j.gim.2022.08.026
A pragmatic clinical trial of cascade testing for familial hypercholesterolemia
Abstract
Purpose: We compared new cases detected per index case in familial hypercholesterolemia (FH) families with or without an identifiable monogenic etiology.
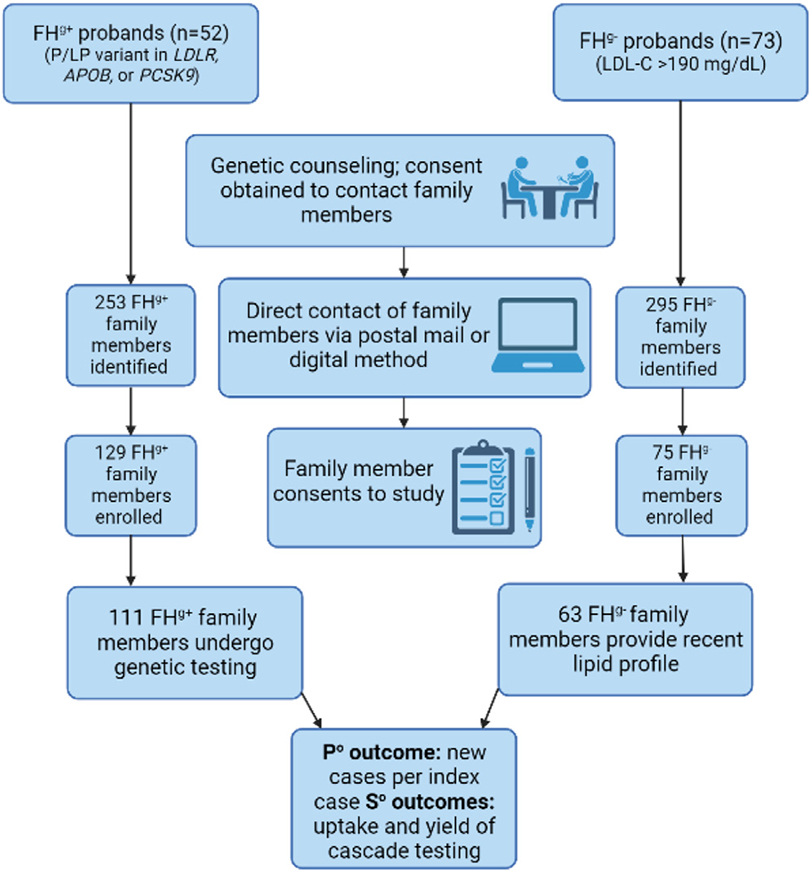
Methods: We enrolled 52 FH probands with a pathogenic variant (FHg+) in LDLR, APOB, or PCSK9 and 73 probands without such a variant (FHg-). After direct contact by the study team, family members (FMs) of FHg+ probands could opt-in for genetic testing and FMs of FHg- probands were asked to provide a lipid profile. New cases were defined as presence of a pathogenic variant in FHg+ families and as low-density lipoprotein cholesterol ≥155 mg/dL in FHg- families.
Results: Of 71 FHg+ probands seen by a genetic counselor, 52 consented and identified 253 FMs (111 consented and were tested, yielding 48 new cases). Of 101 FHg- probands who received counseling, 73 consented and identified 295 FMs (63 consented and were tested, yielding 17 new cases). New case detection per index case was significantly greater in FHg+ than in FHg- families (0.92 vs 0.23), a result of higher cascade testing uptake (43.9 vs 21.4%) and yield (43.2 vs 27.0%) in the former.
Conclusion: New case detection rate was significantly higher in FH families with a monogenic etiology than in those without such an etiology owing to greater uptake and yield of cascade testing.
Trial registration: ClinicalTrials.gov NCT03640234.
Keywords: Cascade testing; Familial hypercholesterolemia; Monogenic; Polygenic; Variant.
Copyright © 2022 American College of Medical Genetics and Genomics. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest The authors declare no conflict of interest.
Figures
Similar articles
-
Lipid phenotype and heritage pattern in families with genetic hypercholesterolemia not related to LDLR, APOB, PCSK9, or APOE.J Clin Lipidol. 2016 Nov-Dec;10(6):1397-1405.e2. doi: 10.1016/j.jacl.2016.09.011. Epub 2016 Sep 22. J Clin Lipidol. 2016. PMID: 27919357
-
Identification of a novel LDLR disease-causing variant using capture-based next-generation sequencing screening of familial hypercholesterolemia patients in Taiwan.Atherosclerosis. 2018 Oct;277:440-447. doi: 10.1016/j.atherosclerosis.2018.08.022. Atherosclerosis. 2018. PMID: 30270083
-
Identification of a novel LDLR p.Glu179Met variant in Thai families with familial hypercholesterolemia and response to treatment with PCSK9 inhibitor.Sci Rep. 2024 Mar 21;14(1):6785. doi: 10.1038/s41598-024-57069-z. Sci Rep. 2024. PMID: 38514665 Free PMC article.
-
Polygenic contribution for familial hypercholesterolemia (FH).Curr Opin Lipidol. 2021 Dec 1;32(6):392-395. doi: 10.1097/MOL.0000000000000787. Curr Opin Lipidol. 2021. PMID: 34751168 Review.
-
Genetic backgrounds and diagnosis of familial hypercholesterolemia.Clin Genet. 2024 Jan;105(1):3-12. doi: 10.1111/cge.14435. Epub 2023 Oct 17. Clin Genet. 2024. PMID: 37849044 Review.
Cited by
-
Genetic testing for familial hypercholesterolemia.Curr Opin Lipidol. 2024 Apr 1;35(2):93-100. doi: 10.1097/MOL.0000000000000925. Epub 2024 Jan 31. Curr Opin Lipidol. 2024. PMID: 38299384 Free PMC article. Review.
-
Innovative Implementation Strategies for Familial Hypercholesterolemia Cascade Testing: The Impact of Genetic Counseling.J Pers Med. 2024 Aug 9;14(8):841. doi: 10.3390/jpm14080841. J Pers Med. 2024. PMID: 39202032 Free PMC article.
-
Utilizing innovative implementation strategies for familial hypercholesterolemia: Implementation outcomes from the IMPACT-FH study.J Clin Lipidol. 2024 Sep-Oct;18(5):e832-e843. doi: 10.1016/j.jacl.2024.07.011. Epub 2024 Jul 31. J Clin Lipidol. 2024. PMID: 39278768
-
IMPACT-FH Study for Implementing Innovative Family Communication and Cascade Testing Strategies for Familial Hypercholesterolemia.JACC Adv. 2024 Aug 14;3(9):101198. doi: 10.1016/j.jacadv.2024.101198. eCollection 2024 Sep. JACC Adv. 2024. PMID: 39238848 Free PMC article.
-
A qualitative study of perceptions of the care pathway for familial hypercholesterolemia: screening, diagnosis, treatment, and family cascade screening.Implement Sci Commun. 2024 Dec 2;5(1):135. doi: 10.1186/s43058-024-00670-0. Implement Sci Commun. 2024. PMID: 39623509 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
