

Systematically higher Ki67 scores on core biopsy samples compared to corresponding resection specimen in breast cancer: a multi-operator and multi-institutional study
- PMID: 35729220
- PMCID: PMC9514990
- DOI: 10.1038/s41379-022-01104-9
Systematically higher Ki67 scores on core biopsy samples compared to corresponding resection specimen in breast cancer: a multi-operator and multi-institutional study
Abstract
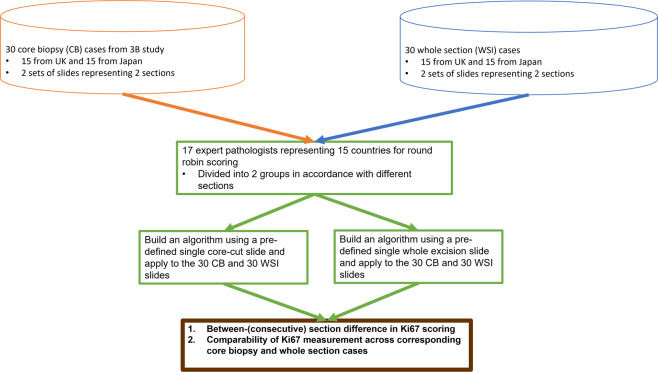
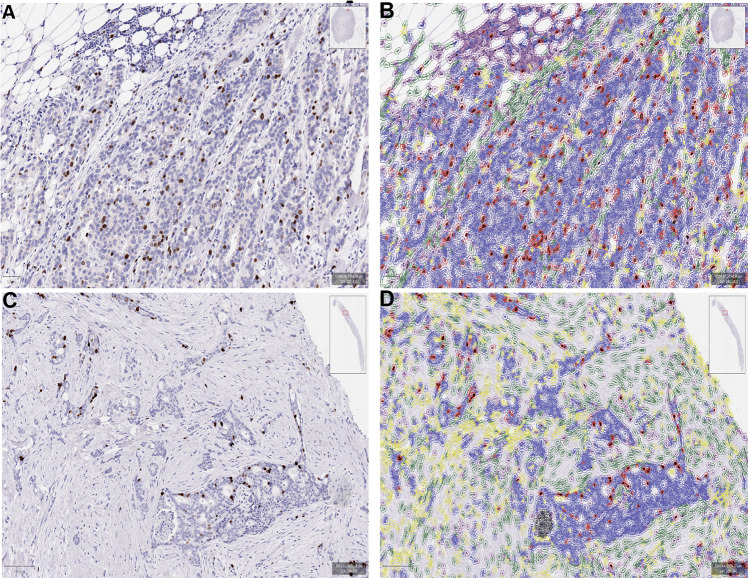
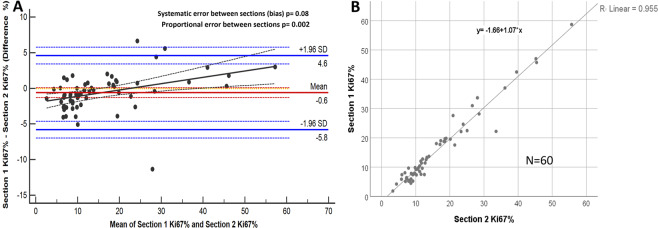
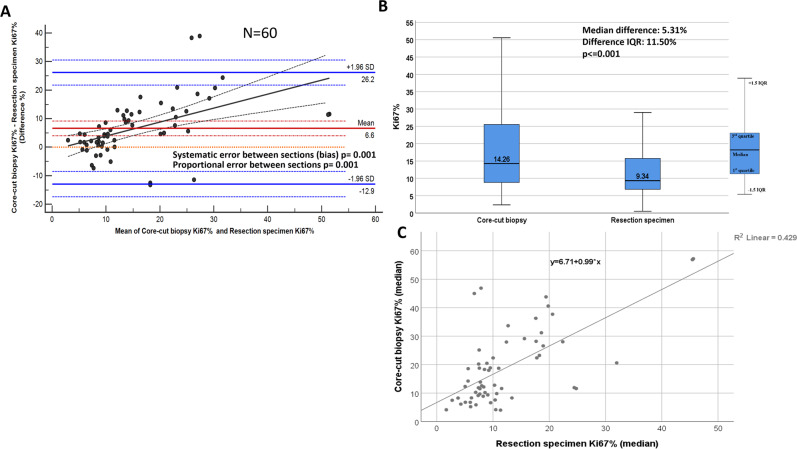
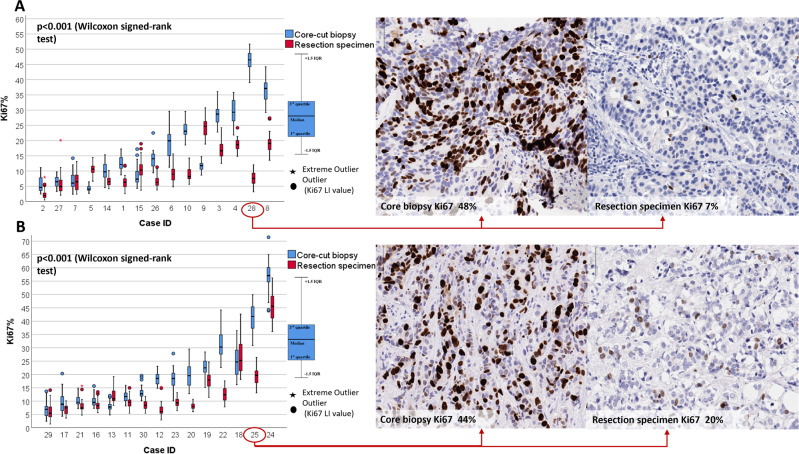
Ki67 has potential clinical importance in breast cancer but has yet to see broad acceptance due to inter-laboratory variability. Here we tested an open source and calibrated automated digital image analysis (DIA) platform to: (i) investigate the comparability of Ki67 measurement across corresponding core biopsy and resection specimen cases, and (ii) assess section to section differences in Ki67 scoring. Two sets of 60 previously stained slides containing 30 core-cut biopsy and 30 corresponding resection specimens from 30 estrogen receptor-positive breast cancer patients were sent to 17 participating labs for automated assessment of average Ki67 expression. The blocks were centrally cut and immunohistochemically (IHC) stained for Ki67 (MIB-1 antibody). The QuPath platform was used to evaluate tumoral Ki67 expression. Calibration of the DIA method was performed as in published studies. A guideline for building an automated Ki67 scoring algorithm was sent to participating labs. Very high correlation and no systematic error (p = 0.08) was found between consecutive Ki67 IHC sections. Ki67 scores were higher for core biopsy slides compared to paired whole sections from resections (p ≤ 0.001; median difference: 5.31%). The systematic discrepancy between core biopsy and corresponding whole sections was likely due to pre-analytical factors (tissue handling, fixation). Therefore, Ki67 IHC should be tested on core biopsy samples to best reflect the biological status of the tumor.
© 2022. The Author(s).
Conflict of interest statement
In the last 12 months, DLR has served as a consultant for advisor to Astra Zeneca, Agendia, Amgen, Cell Signaling Technology, Cepheid, Danaher, Konica-Minolta, Merck, PAIGE.AI, Regeneron, and Sanofi. TON reports a proprietary interest in PAM50/Prosigna and consultant work with Veracyte. JH was former member of the advisory board at Visiopharm A/S. JH has obtained speaker’s honoraria or advisory board remunerations from Roche, Novartis, AstraZeneca, Eli Lilly, Pfizer and MSD. JH is co-founder and shareholder of Stratipath AB. JH has received institutional research grants from Cepheid and Novartis. DFH reports no research or personal financial support related to this study. DFH does report research support unrelated to this study provided to his institution during conduct from Menarini/Silicon BioSystems, Astra Zeneca, Eli Lilly Company, Merrimack Pharmaceuticals, Inc. (Parexel Intl Corp), Veridex and Janssen Diagnostics (Johnson & Johnson), Pfizer, and Puma Biotechnology, Inc. (subcontract Wash Univ St. Louis to Univ Mich). DFH also reports that his institution holds a patent regarding circulating tumor cell characterization for which DFH is the named investigator that was licensed to Menarini Silicon Biosystems and from which both received annual royalties, ending in January 2021. DFH reports personal income related to consulting or advisory board activities from BioVeca, Cellworks, Cepheid, EPIC Sciences, Freenome, Guardant, L-Nutra, Oncocyte, Macrogenics, Predictus BioSciences, Salutogenic Innovations, Turnstone Biologics, and Tempus. DFH reports personally held stock options from InBiomotion. BvdV reports speaker’s honoraria or consultation/advisory board remunerations provided to his institution from Visiopharm, Philips, Merck/MSD and Diaceutics. GV reports receipt of grants/research supports from Roche/Genentech, Ventana Medical Systems, Dako/Agilent Technologies, and receipt of honoraria or consultation fees from Ventana, Dako/Agilent, Roche, MSD Oncology, AstraZeneca, Daiichi Sankyo, Pfizer, Eli Lilly. ZK has served in a paid advisory role to Eli Lilly. Unrelated to this study, SR is currently employed by Stratipath AB. RS reports non-financial support from Merck and Bristol Myers Squibb; research support from Merck, Puma Biotechnology, and Roche; and advisory board fees for Bristol Myers Squibb; and personal fees from Roche for an advisory board related to a trial-research project. RS has no COI related to this project. SF served as expert pathology consultant for Axdev Global Corp inc and as an expert advisory panel for Genomic Health in 2017. RML is co-founder and shareholder of MUSE Microscopy, Inc. and Histolix, Inc. RML served as consultant for Cell IDx, Inc., BriteSeed, Inc., ImmunoPhotonics, Inc., Pathology Watch, Inc. and Verily, Inc. FPL reports board meetings and conference support from Astrazeneca, Lilly, Novartis, Pfizer and Roche. JB served as consultant for Insight Genetics, Inc., BioNTech AG, Biotheranostics, Inc., Pfizer, Rna Diagnostics Inc., oncoXchange/MedcomXchange Communications Inc, Herbert Smith French Solicitors, OncoCyte Corporation. JB served as member of the scientific advisory board for MedcomXchange Communications Inc. JB reports honoraria from NanoString Technologies, Inc., Oncology Education, Biotheranostics, Inc., MedcomXchange Communications Inc. JB reports travel and accommodation expenses support from Biotheranostics, Inc., NanoString Technologies, Inc., Breast Cancer Society of Canada. JB received research funding from Thermo Fisher Scientific, Genoptix, Agendia, NanoString Technologies, Inc., Stratifyer GmbH, Biotheranostics, Inc. The remaining authors declare no competing interests.
Figures
References
-
- Smith I, Robertson J, Kilburn L, Wilcox M, Evans A, Holcombe C, et al. Long-term outcome and prognostic value of Ki67 after perioperative endocrine therapy in postmenopausal women with hormone-sensitive early breast cancer (POETIC): an open-label multicentre parallel-group randomised phase 3 trial. Lancet Oncol 21, 1443–1454 (2020) - PMC - PubMed
-
- Harris LN, Ismaila N, McShane LM, Andre F, Collyar DE, Gonzalez-Angulo AM, et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol 34, 1134–1150 (2016) - PMC - PubMed
-
- Andre F, Ismaila N, Henry NL, Somerfield MR, Bast RC, Barlow W, et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: ASCO Clinical Practice Guideline Update-Integration of Results From TAILORx. J Clin Oncol 37, 1956–1964 (2019) - PubMed
