

Management of toxicities associated with targeted therapies for HR-positive metastatic breast cancer: a multidisciplinary approach is the key to success
- PMID: 31065872
- PMCID: PMC6586706
- DOI: 10.1007/s10549-019-05261-5
Management of toxicities associated with targeted therapies for HR-positive metastatic breast cancer: a multidisciplinary approach is the key to success
Abstract
Purpose: Agents targeting HR-positive, HER2-negative locally advanced or metastatic breast cancer have improved patient outcomes compared with conventional single-agent endocrine therapy. Currently, approved targeted agents include everolimus and three CDK4/6 inhibitors, palbociclib, ribociclib, and abemaciclib. Unlike the well-characterized and easily manageable safety profile of endocrine therapies, adverse events associated with targeted therapies are complex and potentially severe. Their prompt recognition and treatment, crucial for prolonged endocrine sensitivity and survival, may be challenging and requires a multidisciplinary effort and a good knowledge of drug interactions.
Methods: We reviewed the current evidence on the drug safety of targeted agents for metastatic breast cancer currently used in clinical practice in Italy, supported by the clinical experience of Italian oncologists with expertise in the field.
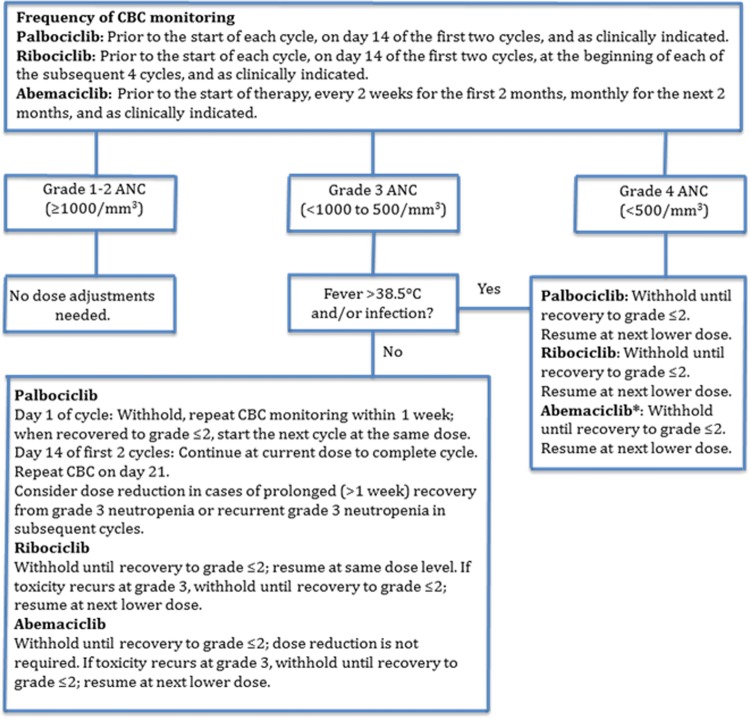
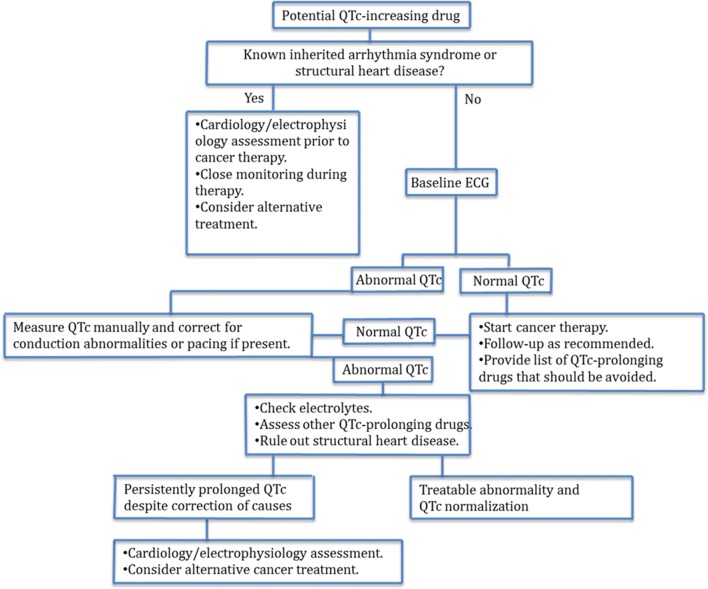
Results: All oncologists had used CDK4/6 inhibitors in clinical practice and/or within a clinical trial. The clinical management of toxicities, including dose adjustments, treatment interruptions, and concerns regarding special populations is discussed, and the management of relevant adverse events, related to individual agents and class-specific, toxicities is reviewed. Hematologic toxicities have the greatest impact on clinical management of the disease and on patients. Although toxicities associated with the new treatments result in more visits to the physician and more time and attention with patients, they are manageable, with no need for the oncologist to consult with specialist physicians.
Conclusions: Based on the available evidence and current guidelines, we propose a series of practical recommendations for multidisciplinary clinical management of the various toxicities associated with the addition of targeted agents to endocrine therapy.
Keywords: Abemaciclib; Advanced breast cancer; Everolimus; Neutropenia; Palbociclib; Ribociclib.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Cristofanilli M, Turner NC, Bondarenko I, Ro J, Im SA, Masuda N, Colleoni M, DeMichele A, Loi S, Verma S, Iwata H, Harbeck N, Zhang K, Theall KP, Jiang Y, Bartlett CH, Koehler M, Slamon D. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016;17(4):425–439. - PubMed
-
- Finn RS, Martin M, Rugo HS, Jones S, Im SA, Gelmon K, Harbeck N, Lipatov ON, Walshe JM, Moulder S, Gauthier E, Lu DR, Randolph S, Dieras V, Slamon DJ. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375(20):1925–1936. - PubMed
-
- Goetz MP, Toi M, Campone M, Sohn J, Paluch-Shimon S, Huober J, Park IH, Tredan O, Chen SC, Manso L, Freedman OC, Garnica Jaliffe G, Forrester T, Frenzel M, Barriga S, Smith IC, Bourayou N, Di Leo A. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J Clin Oncol. 2017;35(32):3638–3646. - PubMed
-
- Hortobagyi GN, Stemmer SM, Burris HA, Yap YS, Sonke GS, Paluch-Shimon S, Campone M, Petrakova K, Blackwell KL, Winer EP, Janni W, Verma S, Conte P, Arteaga CL, Cameron DA, Mondal S, Su F, Miller M, Elmeliegy M, Germa C, O’Shaughnessy J. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol. 2018;29(7):1541–1547. - PubMed
-
- Royce M, Bachelot T, Villanueva C, Ozguroglu M, Azevedo SJ, Cruz FM, Debled M, Hegg R, Toyama T, Falkson C, Jeong J, Srimuninnimit V, Gradishar WJ, Arce C, Ridolfi A, Lin C, Cardoso F. Everolimus plus endocrine therapy for postmenopausal women with estrogen receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: a clinical trial. JAMA Oncol. 2018;4(7):977–984. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
