

Effect of generalised access to early diagnosis and treatment and targeted mass drug administration on Plasmodium falciparum malaria in Eastern Myanmar: an observational study of a regional elimination programme
- PMID: 29703425
- PMCID: PMC5946089
- DOI: 10.1016/S0140-6736(18)30792-X
Effect of generalised access to early diagnosis and treatment and targeted mass drug administration on Plasmodium falciparum malaria in Eastern Myanmar: an observational study of a regional elimination programme
Abstract
Background: Potentially untreatable Plasmodium falciparum malaria threatens the Greater Mekong subregion. A previous series of pilot projects in Myanmar, Laos, Cambodia, and Vietnam suggested that mass drug administration was safe, and when added to provision of early diagnosis and treatment, could reduce the reservoir of P falciparum and interrupts transmission. We examined the effects of a scaled-up programme of this strategy in four townships of eastern Myanmar on the incidence of P falciparum malaria.
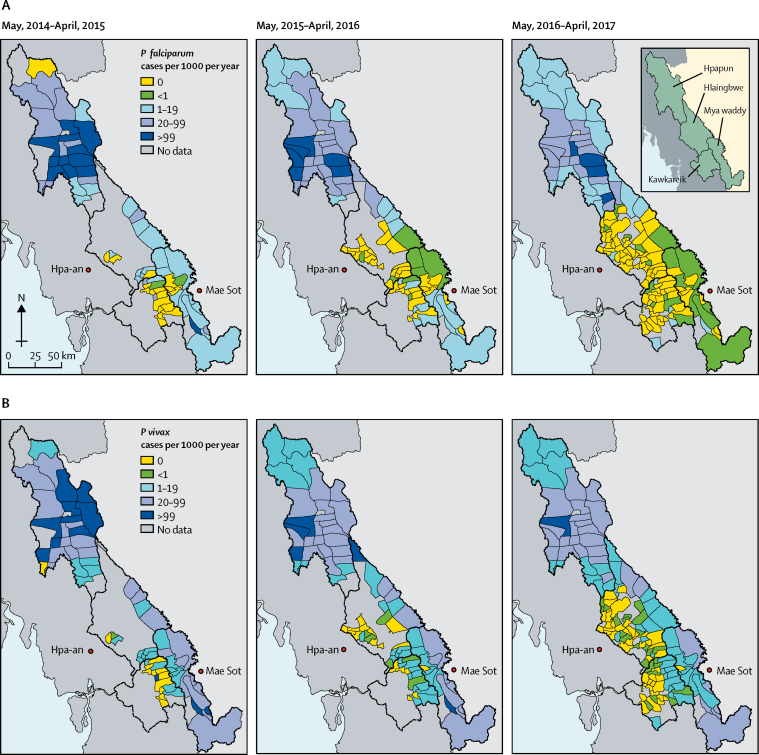
Methods: The programme was implemented in the four townships of Myawaddy, Kawkareik, Hlaingbwe, and Hpapun in Kayin state, Myanmar. Increased access to early diagnosis and treatment of malaria was provided to all villages through community-based malaria posts equipped with rapid diagnostic tests, and treatment with artemether-lumefantrine plus single low-dose primaquine. Villages were identified as malarial hotspots (operationally defined as >40% malaria, of which 20% was P falciparum) with surveys using ultrasensitive quantitative PCR either randomly or targeted at villages where the incidence of clinical cases of P falciparum malaria remained high (ie, >100 cases per 1000 individuals per year) despite a functioning malaria post. During each survey, a 2 mL sample of venous blood was obtained from randomly selected adults. Hotspots received targeted mass drug administration with dihydroartemisinin-piperaquine plus single-dose primaquine once per month for 3 consecutive months in addition to the malaria posts. The main outcome was the change in village incidence of clinical P falciparum malaria, quantified using a multivariate, generalised, additive multilevel model. Malaria prevalence was measured in the hotspots 12 months after mass drug administration.
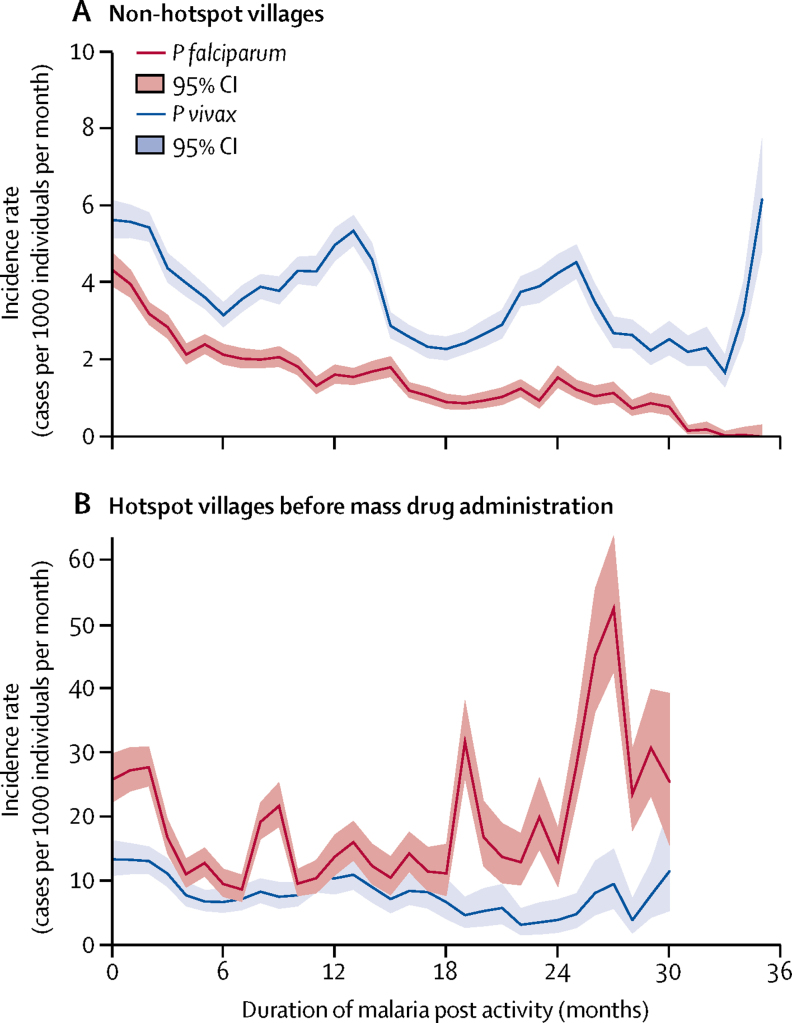
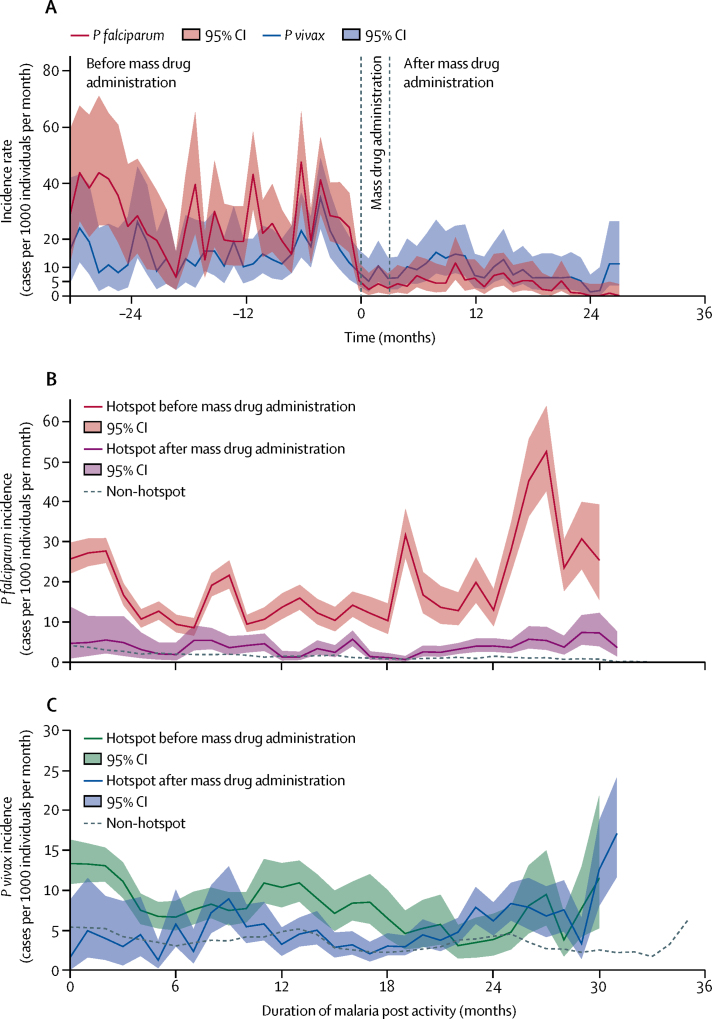
Findings: Between May 1, 2014, and April 30, 2017, 1222 malarial posts were opened, providing early diagnosis and treatment to an estimated 365 000 individuals. Incidence of P falciparum malaria decreased by 60 to 98% in the four townships. 272 prevalence surveys were undertaken and 69 hotspot villages were identified. By April 2017, 50 hotspots were treated with mass drug administration. Hotspot villages had a three times higher incidence of P falciparum at malarial posts than neighbouring villages (adjusted incidence rate ratio [IRR] 2·7, 95% CI 1·8-4·4). Early diagnosis and treatment was associated with a significant decrease in P falciparum incidence in hotspots (IRR 0·82, 95% CI 0·76-0·88 per quarter) and in other villages (0·75, 0·73-0·78 per quarter). Mass drug administration was associated with a five-times decrease in P falciparum incidence within hotspot villages (IRR 0·19, 95% CI 0·13-0·26). By April, 2017, 965 villages (79%) of 1222 corresponding to 104 village tracts were free from P falciparum malaria for at least 6 months. The prevalence of wild-type genotype for K13 molecular markers of artemisinin resistance was stable over the three years (39%; 249/631).
Interpretation: Providing early diagnosis and effective treatment substantially decreased village-level incidence of artemisinin-resistant P falciparum malaria in hard-to-reach, politically sensitive regions of eastern Myanmar. Targeted mass drug administration significantly reduced malaria incidence in hotspots. If these activities could proceed in all contiguous endemic areas in addition to standard control programmes already implemented, there is a possibility of subnational elimination of P falciparum.
Funding: The Bill & Melinda Gates Foundation, the Regional Artemisinin Initiative (Global Fund against AIDS, Tuberculosis and Malaria), and the Wellcome Trust.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Can improving access to care help to eliminate malaria?Lancet. 2018 May 12;391(10133):1870-1871. doi: 10.1016/S0140-6736(18)30910-3. Epub 2018 Apr 24. Lancet. 2018. PMID: 29703426 No abstract available.
References
-
- Imwong M, Hien TT, Thuy-Nhien NT, Dondorp AM, White NJ. Spread of a single multidrug resistant malaria parasite lineage (PfPailin) to Vietnam. Lancet Infect Dis. 2017;17:1022–1023. - PubMed
-
- WHO . World Health Organization; Geneva: 2016. Eliminating malaria in the Greater Mekong subregion: united to end a deadly disease.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
