

Guideline Application in Real world: multi-Institutional Based survey of Adjuvant and first-Line pancreatic Ductal adenocarcinoma treatment in Italy. Primary analysis of the GARIBALDI survey
- PMID: 36731325
- PMCID: PMC10024128
- DOI: 10.1016/j.esmoop.2022.100777
Guideline Application in Real world: multi-Institutional Based survey of Adjuvant and first-Line pancreatic Ductal adenocarcinoma treatment in Italy. Primary analysis of the GARIBALDI survey
Abstract
Background: Information about the adherence to scientific societies guidelines in the 'real-world' therapeutic management of oncological patients are lacking. This multicenter, prospective survey was aimed to improve the knowledge relative to 2017-2018 recommendations of the Italian Association of Medical Oncology (AIOM).
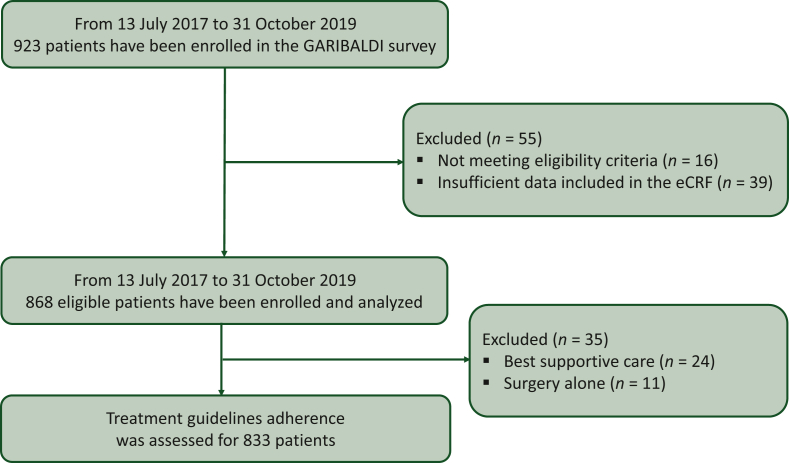
Patients and methods: Treatment-naive adult patients with pancreatic adenocarcinoma were enrolled. Group A received adjuvant therapy, group B received primary chemotherapy, and group C had metastatic disease. The results on patients accrued until 31 October 2019 with a mature follow-up were presented.
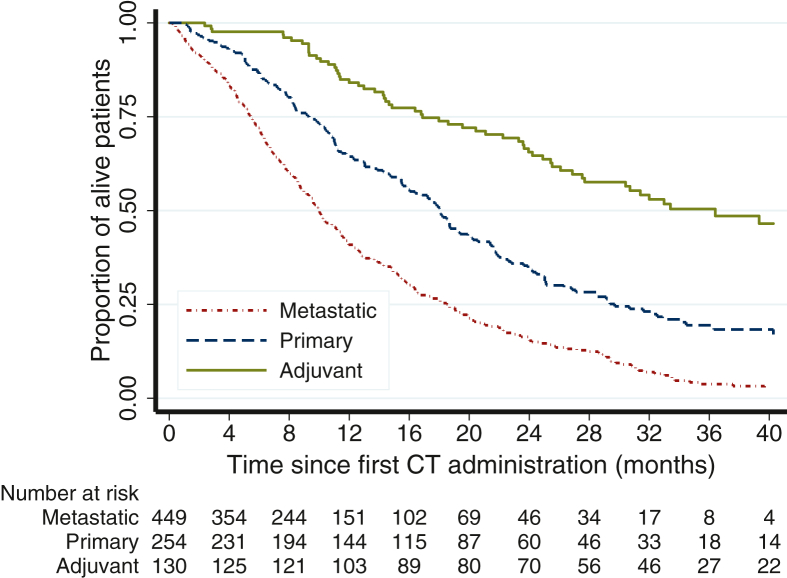
Results: Since July 2017, 833 eligible patients of 923 (90%) were enrolled in 44 Italian centers. The median age was 69 years (range 36-89 years; 24% >75 years); 48% were female; 93% had Eastern Cooperative Oncology Group (ECOG) performance status (PS) score of 0 or 1; group A: 16%, group B: 30%; group C: 54%; 72% Nord, 13% Center, 15% South. In group A, guidelines adherence was 68% [95% confidence interval (CI) 59% to 76%]; 53% of patients received gemcitabine and 15% gemcitabine + capecitabine; median CA19.9 was 29 (range 0-7300; not reported 15%); median survival was 36.4 months (95% CI 27.5-47.3 months). In group B, guidelines adherence was 96% (95% CI 92% to 98%); 55% of patients received nab-paclitaxel + gemcitabine, 27% FOLFIRINOX, 12% gemcitabine, and 3% clinical trial; median CA19.9 was 337 (range 0-20220; not reported 9%); median survival was 18.1 months (95% CI 15.6-19.9 months). In group C, guidelines adherence was 96% (95% CI 94% to 98%); 71% of patients received nab-paclitaxel + gemcitabine, 16% gemcitabine, 8% FOLFIRINOX, and 4% clinical trial; liver and lung metastases were reported in 76% and 23% of patients, respectively; median CA19.9 value was 760 (range 0-1374500; not reported 9%); median survival was 10.0 months (95% CI 9.1-11.1 months).
Conclusions: The GARIBALDI survey shows a very high rate of adherence to guidelines and survival outcome in line with the literature. CA19.9 testing should be enhanced; nutritional and psychological counseling represent an unmet need. Enrollment to assess adherence to updated AIOM guidelines is ongoing.
Keywords: adherence to guidelines; adjuvant; first line; pancreatic adenocarcinoma; prospective survey.
Copyright © 2023 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure RM declares grants or contracts from AstraZeneca and participation on a Data Safety Monitoring Board or Advisory Board for Eli Lilly, PANAVANCE, Celgene, AstraZeneca, Viatris, Merck Sharp & Dohme, Servier, SOTIO, and Baxter. BF declares payment for consulting fees from Servier and AAA Novartis and payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Eli Lilly, MSD, EISAI, and Bayer. MM declares grants or contracts from Roche and Novartis, payment for consulting fees from Viatris, AstraZeneca, MSD, and Merck; payment for participation on a Data Safety Monitoring Board or Advisory Board from Novartis. CL declares payment for consulting fees from Astrazeneca e Merck and support for attending meetings and/or travel from Pfizer, Ipsen and Celgene. DMMC declares payment for participation on a Data Safety Monitoring Board or Advisory Board from OncoSil and Olaparib and for Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid from Editorial Board Future Oncology. SM declares payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Eli Lilly, Roche, Pfizer, Janssen, Italfarmaco, and BMS and for participation on a Data Safety Monitoring Board or Advisory Board from Eli Lilly, Merck, Pfizer, Janssen, and BMS; payment or has a leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid from AIOM Sicilia. GE declares payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Viatris, Amgen, and AstraZeneca and support for attending meetings and/or travel from Ipsen and Viatris. SC declares payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Amgen, Merk, Servier, Bayer, and Sanofi and support for attending meetings and/or travel from Amgen, Merk, and Servier. GGC declares payment for attending meetings and/or travel from Incyte, Eli Lilly, Amgen, and MSD and for the participation on a Data Safety Monitoring Board or Advisory Board for Eli Lilly, MSD, and AstraZeneca. ME declares payment for consulting fees from MSD. GM declares consulting fees from Italfarmaco, payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Roche, Merck, Eli Lilly, Servier, and Amgen. PL declares consulting fees from Ipsen and Italfarmaco. CP declares institutional grants from Ely Lilly, Bayer, and Roche; consulting fees from BMS, Ely Lilly, Novartis, and Merck and for the participation on a Data Safety Monitoring Board or Advisory Board for BMS, Amgen, and Novartis. All other authors have declared no conflicts of interest.
Figures
References
-
- Reni M., Zanon S., Balzano G., et al. Selecting patients for resection after primary chemotherapy for non-metastatic pancreatic adenocarcinoma. Ann Oncol. 2017;28:2786–2792. - PubMed
-
- Oettle H., Post S., Neuhaus P., et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297:267–277. - PubMed
-
- Neoptolemos J.P., Palmer D.H., Ghaneh P., et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet. 2017;389:1011–1024. - PubMed
-
- Conroy T., Hammel P., Hebbar M., et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med. 2018;379:2395–2406. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
