

Prostate Cancer Screening With PSA, Kallikrein Panel, and MRI: The ProScreen Randomized Trial
- PMID: 38581254
- PMCID: PMC10999002
- DOI: 10.1001/jama.2024.3841
Prostate Cancer Screening With PSA, Kallikrein Panel, and MRI: The ProScreen Randomized Trial
Abstract
Importance: Prostate-specific antigen (PSA) screening has potential to reduce prostate cancer mortality but frequently detects prostate cancer that is not clinically important.
Objective: To describe rates of low-grade (grade group 1) and high-grade (grade groups 2-5) prostate cancer identified among men invited to participate in a prostate cancer screening protocol consisting of a PSA test, a 4-kallikrein panel, and a magnetic resonance imaging (MRI) scan.
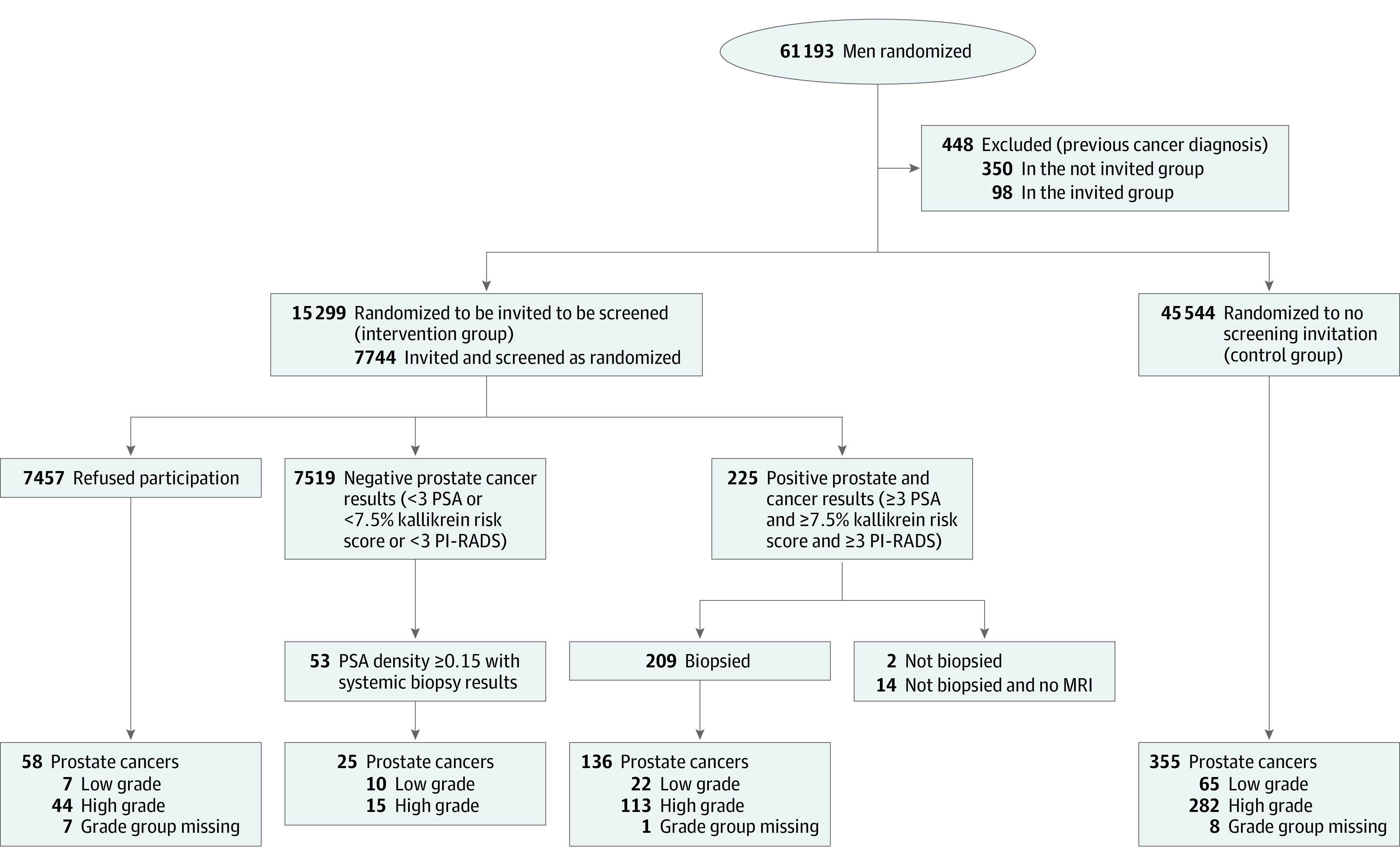
Design, setting, and participants: The ProScreen trial is a clinical trial conducted in Helsinki and Tampere, Finland, that randomized 61 193 men aged 50 through 63 years who were free of prostate cancer in a 1:3 ratio to either be invited or not be invited to undergo screening for prostate cancer between February 2018 and July 2020.
Interventions: Participating men randomized to the intervention underwent PSA testing. Those with a PSA level of 3.0 ng/mL or higher underwent additional testing for high-grade prostate cancer with a 4-kallikrein panel risk score. Those with a kallikrein panel score of 7.5% or higher underwent an MRI of the prostate gland, followed by targeted biopsies for those with abnormal prostate gland MRI findings. Final data collection occurred through June 31, 2023.
Main outcomes and measures: In descriptive exploratory analyses, the cumulative incidence of low-grade and high-grade prostate cancer after the first screening round were compared between the group invited to undergo prostate cancer screening and the control group.
Results: Of 60 745 eligible men (mean [SD] age, 57.2 [4.0] years), 15 201 were randomized to be invited and 45 544 were randomized not to be invited to undergo prostate cancer screening. Of 15 201 eligible males invited to undergo screening, 7744 (51%) participated. Among them, 32 low-grade prostate cancers (cumulative incidence, 0.41%) and 128 high-grade prostate cancers (cumulative incidence, 1.65%) were detected, with 1 cancer grade group result missing. Among the 7457 invited men (49%) who refused participation, 7 low-grade prostate cancers (cumulative incidence, 0.1%) and 44 high-grade prostate cancers (cumulative incidence, 0.6%) were detected, with 7 cancer grade groups missing. For the entire invited screening group, 39 low-grade prostate cancers (cumulative incidence, 0.26%) and 172 high-grade prostate cancers (cumulative incidence, 1.13%) were detected. During a median follow-up of 3.2 years, in the group not invited to undergo screening, 65 low-grade prostate cancers (cumulative incidence, 0.14%) and 282 high-grade prostate cancers (cumulative incidence, 0.62%) were detected. The risk difference for the entire group randomized to the screening invitation vs the control group was 0.11% (95% CI, 0.03%-0.20%) for low-grade and 0.51% (95% CI, 0.33%-0.70%) for high-grade cancer.
Conclusions and relevance: In this preliminary descriptive report from an ongoing randomized clinical trial, 1 additional high-grade cancer per 196 men and 1 low-grade cancer per 909 men were detected among those randomized to be invited to undergo a single prostate cancer screening intervention compared with those not invited to undergo screening. These preliminary findings from a single round of screening should be interpreted cautiously, pending results of the study's primary mortality outcome.
Trial registration: ClinicalTrials.gov Identifier: NCT03423303.
Conflict of interest statement
Figures

Comment on
-
A Pragmatic Approach to Prostate Cancer Screening.JAMA. 2024 May 7;331(17):1448-1450. doi: 10.1001/jama.2024.4089. JAMA. 2024. PMID: 38581253 No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
