

Deploying unsupervised clustering analysis to derive clinical phenotypes and risk factors associated with mortality risk in 2022 critically ill patients with COVID-19 in Spain
- PMID: 33588914
- PMCID: PMC7883885
- DOI: 10.1186/s13054-021-03487-8
Deploying unsupervised clustering analysis to derive clinical phenotypes and risk factors associated with mortality risk in 2022 critically ill patients with COVID-19 in Spain
Abstract
Background: The identification of factors associated with Intensive Care Unit (ICU) mortality and derived clinical phenotypes in COVID-19 patients could help for a more tailored approach to clinical decision-making that improves prognostic outcomes.
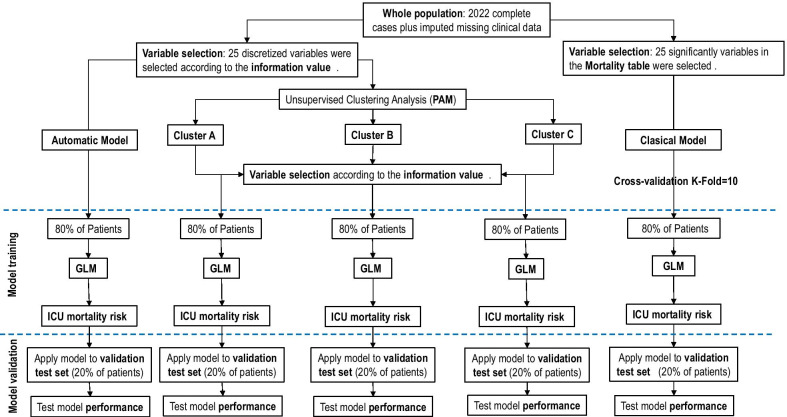
Methods: Prospective, multicenter, observational study of critically ill patients with confirmed COVID-19 disease and acute respiratory failure admitted from 63 ICUs in Spain. The objective was to utilize an unsupervised clustering analysis to derive clinical COVID-19 phenotypes and to analyze patient's factors associated with mortality risk. Patient features including demographics and clinical data at ICU admission were analyzed. Generalized linear models were used to determine ICU morality risk factors. The prognostic models were validated and their performance was measured using accuracy test, sensitivity, specificity and ROC curves.
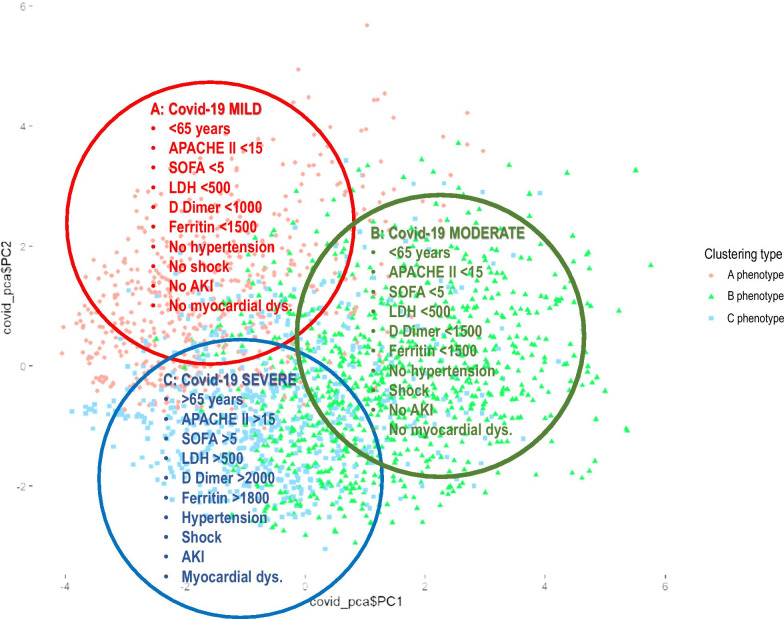
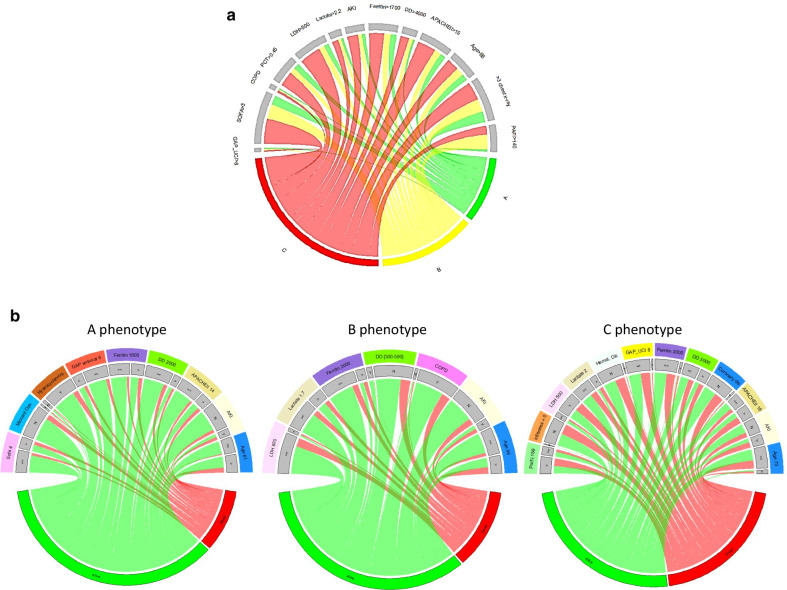
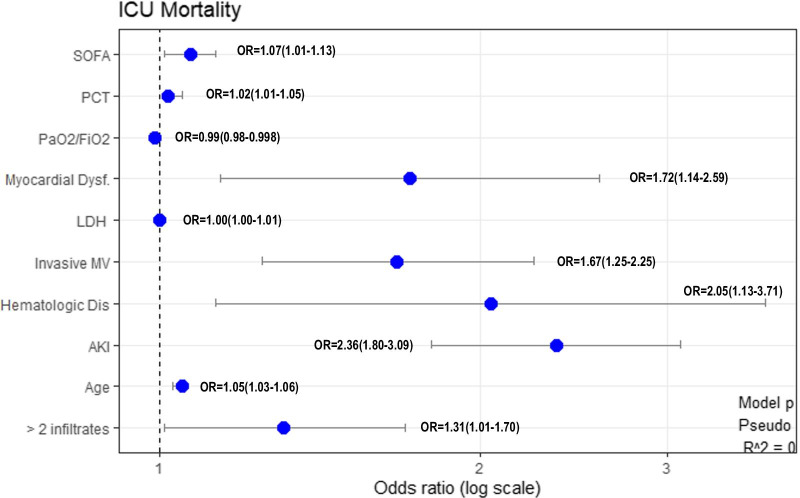
Results: The database included a total of 2022 patients (mean age 64 [IQR 5-71] years, 1423 (70.4%) male, median APACHE II score (13 [IQR 10-17]) and SOFA score (5 [IQR 3-7]) points. The ICU mortality rate was 32.6%. Of the 3 derived phenotypes, the A (mild) phenotype (537; 26.7%) included older age (< 65 years), fewer abnormal laboratory values and less development of complications, B (moderate) phenotype (623, 30.8%) had similar characteristics of A phenotype but were more likely to present shock. The C (severe) phenotype was the most common (857; 42.5%) and was characterized by the interplay of older age (> 65 years), high severity of illness and a higher likelihood of development shock. Crude ICU mortality was 20.3%, 25% and 45.4% for A, B and C phenotype respectively. The ICU mortality risk factors and model performance differed between whole population and phenotype classifications.
Conclusion: The presented machine learning model identified three clinical phenotypes that significantly correlated with host-response patterns and ICU mortality. Different risk factors across the whole population and clinical phenotypes were observed which may limit the application of a "one-size-fits-all" model in practice.
Keywords: Machine learning; Phenotypes; Prognosis; Risk factors; Severe SARS-CoV-2 infection.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
References
-
- https://coronavirus.jhu.edu/map.html. Accessed 28 November 2020
-
- Actualización nº 291. Enfermedad por el coronavirus (COVID- 19). Ministerio de Sanidad de España. https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual...
-
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, the Northwell COVID-19 Research Consortium et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052–2059. doi: 10.1001/jama.2020.6775. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
