

Cooking with liquefied petroleum gas or biomass and fetal growth outcomes: a multi-country randomised controlled trial
- PMID: 38614630
- PMCID: PMC11027158
- DOI: 10.1016/S2214-109X(24)00033-0
Cooking with liquefied petroleum gas or biomass and fetal growth outcomes: a multi-country randomised controlled trial
Erratum in
-
Correction to Lancet Glob Health 2024; 12: e815-25.Lancet Glob Health. 2024 Jul;12(7):e1093. doi: 10.1016/S2214-109X(24)00223-7. Epub 2024 May 29. Lancet Glob Health. 2024. PMID: 38823409 Free PMC article. No abstract available.
Abstract
Background: Household air pollution might lead to fetal growth restriction during pregnancy. We aimed to investigate whether a liquefied petroleum gas (LPG) intervention to reduce personal exposures to household air pollution during pregnancy would alter fetal growth.
Methods: The Household Air Pollution Intervention Network (HAPIN) trial was an open-label randomised controlled trial conducted in ten resource-limited settings across Guatemala, India, Peru, and Rwanda. Pregnant women aged 18-34 years (9-19 weeks of gestation) were randomly assigned in a 1:1 ratio to receive an LPG stove, continuous fuel delivery, and behavioural messaging or to continue usual cooking with biomass for 18 months. We conducted ultrasound assessments at baseline, 24-28 weeks of gestation (the first pregnancy visit), and 32-36 weeks of gestation (the second pregnancy visit), to measure fetal size; we monitored 24 h personal exposures to household air pollutants during these visits; and we weighed children at birth. We conducted intention-to-treat analyses to estimate differences in fetal size between the intervention and control group, and exposure-response analyses to identify associations between household air pollutants and fetal size. This trial is registered with ClinicalTrials.gov (NCT02944682).
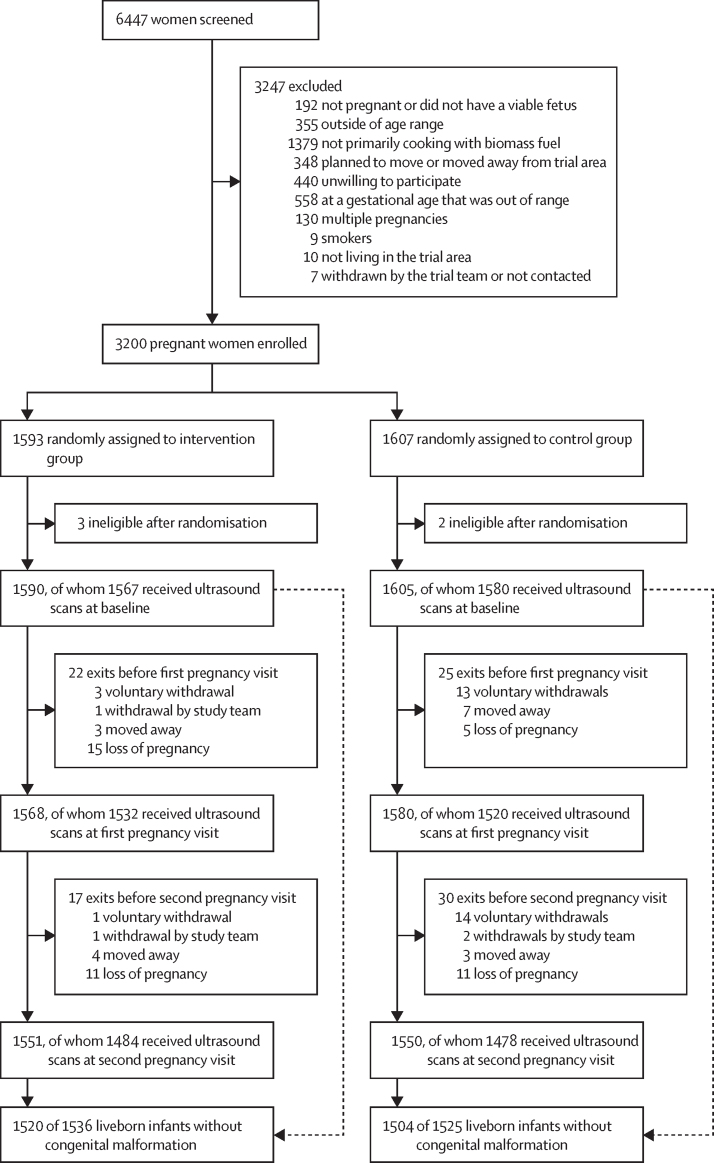
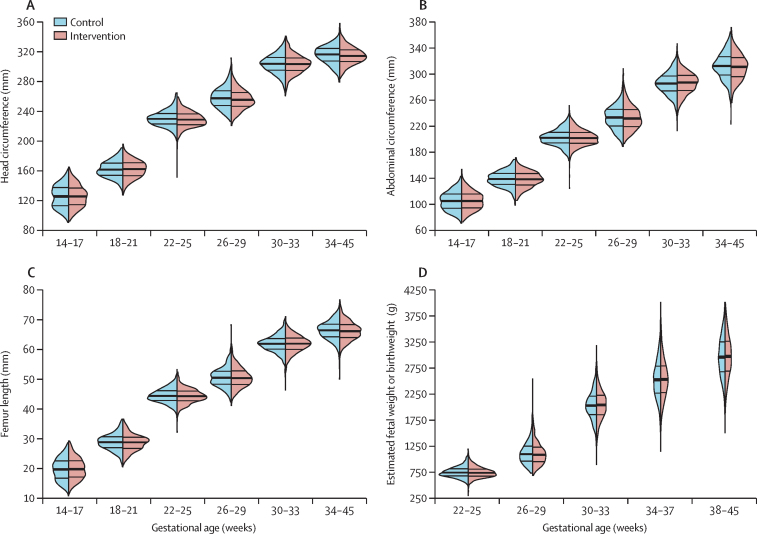
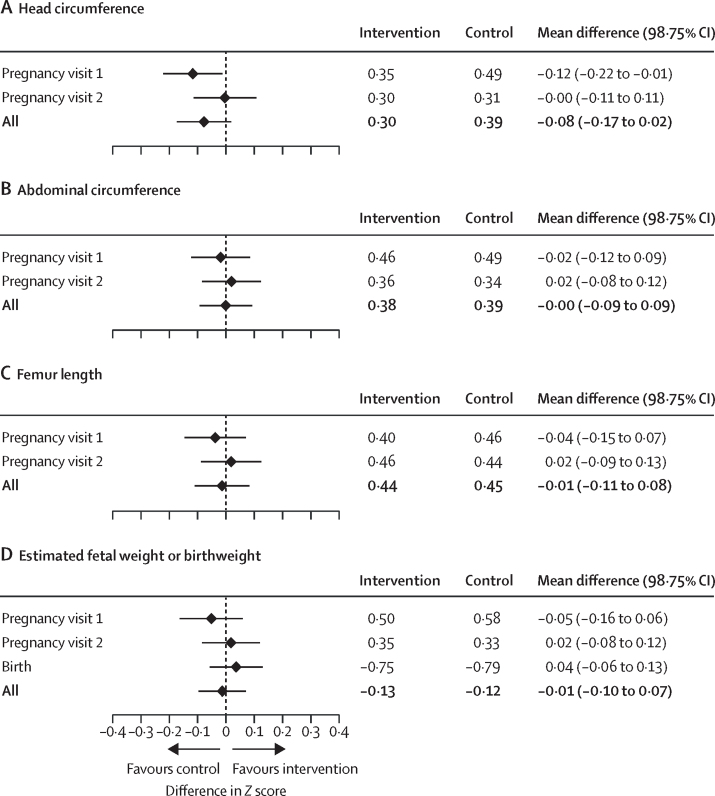
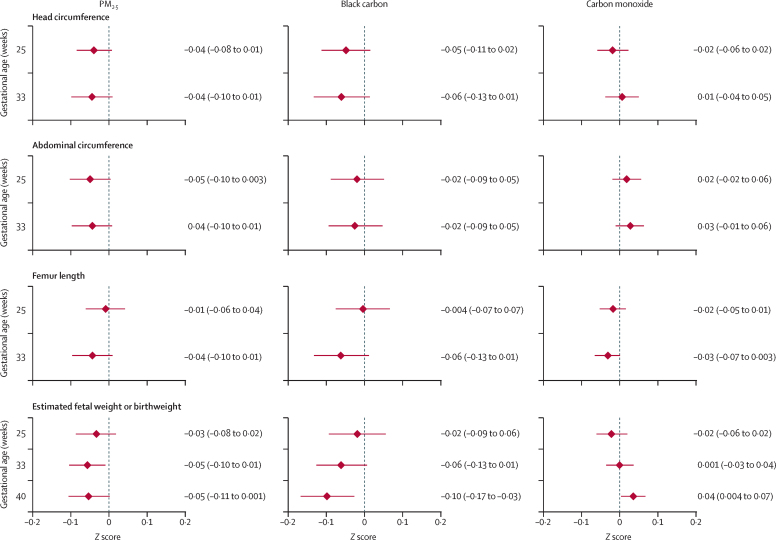
Findings: Between May 7, 2018, and Feb 29, 2020, we randomly assigned 3200 pregnant women (1593 to the intervention group and 1607 to the control group). The mean gestational age was 14·5 (SD 3·0) weeks and mean maternal age was 25·6 (4·5) years. We obtained ultrasound assessments in 3147 (98·3%) women at baseline, 3052 (95·4%) women at the first pregnancy visit, and 2962 (92·6%) at the second pregnancy visit, through to Aug 25, 2020. Intervention adherence was high (the median proportion of days with biomass stove use was 0·0%, IQR 0·0-1·6) and pregnant women in the intervention group had lower mean exposures to particulate matter with a diameter less than 2·5 μm (PM2·5; 35·0 [SD 37·2] μg/m3vs 103·3 [97·9] μg/m3) than did women in the control group. We did not find differences in averaged post-randomisation Z scores for head circumference (0·30 vs 0·39; p=0·04), abdominal circumference (0·38 vs 0·39; p=0·99), femur length (0·44 vs 0·45; p=0·73), and estimated fetal weight or birthweight (-0·13 vs -0·12; p=0·70) between the intervention and control groups. Personal exposures to household air pollutants were not associated with fetal size.
Interpretation: Although an LPG cooking intervention successfully reduced personal exposure to air pollution during pregnancy, it did not affect fetal size. Our findings do not support the use of unvented liquefied petroleum gas stoves as a strategy to increase fetal growth in settings were biomass fuels are used predominantly for cooking.
Funding: US National Institutes of Health and Bill & Melinda Gates Foundation.
Translations: For the Kinyarwanda, Spanish and Tamil translations of the abstract see Supplementary Materials section.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests LW reports a grant from the US National Institute of Environmental Health Sciences. All other authors declare no competing interests.
Figures
Comment in
-
Increasing women's access to household environments free from air pollution during pregnancy.Lancet Glob Health. 2024 May;12(5):e723-e724. doi: 10.1016/S2214-109X(24)00137-2. Lancet Glob Health. 2024. PMID: 38614620 No abstract available.
References
-
- Bennitt FB, Wozniak SS, Causey K, Burkart K, Brauer M, GBD Risk Factor Collaborators Estimating disease burden attributable to household air pollution: new methods within the Global Burden of Disease Study. Lancet Glob Health. 2021;9:S18.
-
- Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379:2162–2172. - PubMed
-
- National Collaborating Centre for Women's and Children's Health . RCOG Press; London: March, 2008. Antenatal care: routine care for the healthy pregnant woman. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
