

Earlier versus later start of antiretroviral therapy in HIV-infected adults with tuberculosis
- PMID: 22010913
- PMCID: PMC4879711
- DOI: 10.1056/NEJMoa1013911
Earlier versus later start of antiretroviral therapy in HIV-infected adults with tuberculosis
Abstract
Background: Tuberculosis remains an important cause of death among patients infected with the human immunodeficiency virus (HIV). Robust data are lacking with regard to the timing for the initiation of antiretroviral therapy (ART) in relation to the start of antituberculosis therapy.
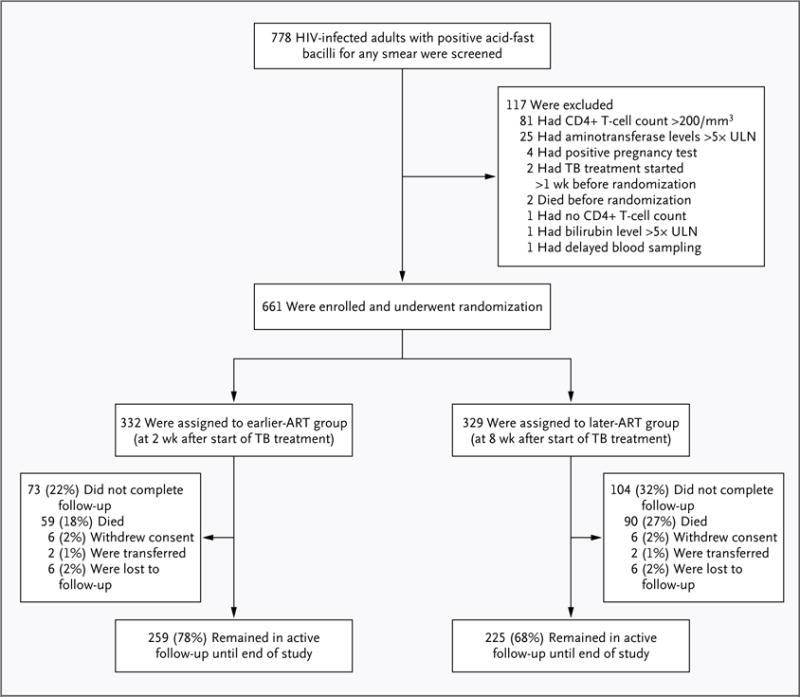
Methods: We tested the hypothesis that the timing of ART initiation would significantly affect mortality among adults not previously exposed to antiretroviral drugs who had newly diagnosed tuberculosis and CD4+ T-cell counts of 200 per cubic millimeter or lower. After beginning the standard, 6-month treatment for tuberculosis, patients were randomly assigned to either earlier treatment (2 weeks after beginning tuberculosis treatment) or later treatment (8 weeks after) with stavudine, lamivudine, and efavirenz. The primary end point was survival.
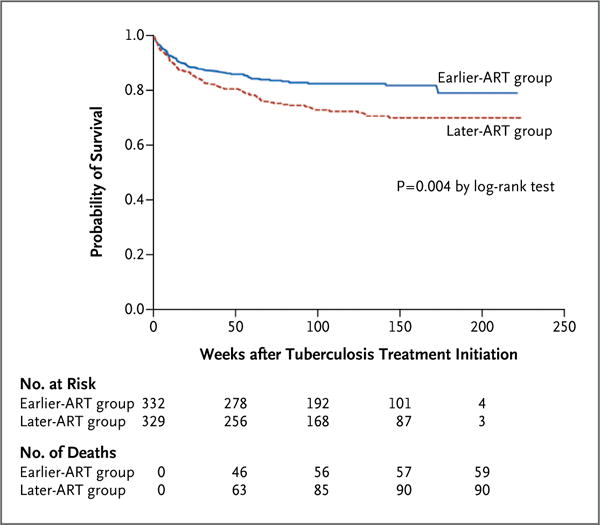
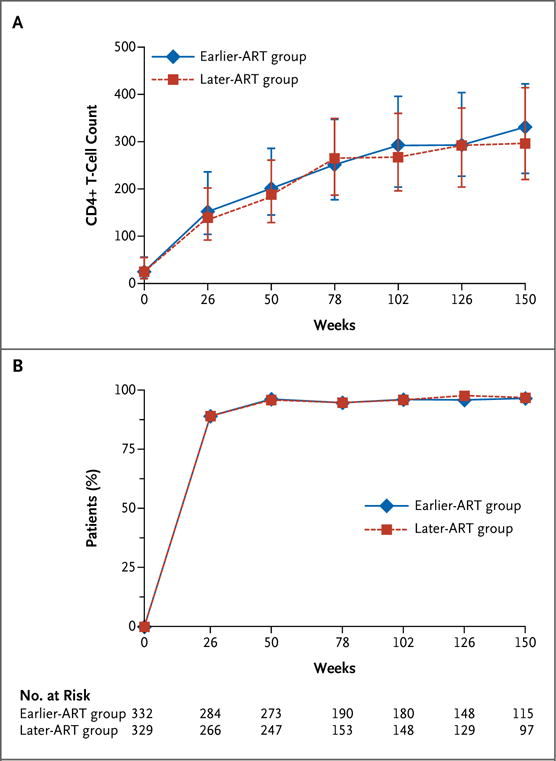
Results: A total of 661 patients were enrolled and were followed for a median of 25 months. The median CD4+ T-cell count was 25 per cubic millimeter, and the median viral load was 5.64 log(10) copies per milliliter. The risk of death was significantly reduced in the group that received ART earlier, with 59 deaths among 332 patients (18%), as compared with 90 deaths among 329 patients (27%) in the later-ART group (hazard ratio, 0.62; 95% confidence interval [CI]; 0.44 to 0.86; P=0.006). The risk of tuberculosis-associated immune reconstitution inflammatory syndrome was significantly increased in the earlier-ART group (hazard ratio, 2.51; 95% CI, 1.78 to 3.59; P<0.001). Irrespective of the study group, the median gain in the CD4+ T-cell count was 114 per cubic millimeter, and the viral load was undetectable at week 50 in 96.5% of the patients.
Conclusions: Initiating ART 2 weeks after the start of tuberculosis treatment significantly improved survival among HIV-infected adults with CD4+ T-cell counts of 200 per cubic millimeter or lower. (Funded by the French National Agency for Research on AIDS and Viral Hepatitis and the National Institutes of Health; CAMELIA ClinicalTrials.gov number, NCT01300481.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
When to start antiretroviral therapy in HIV-associated tuberculosis.N Engl J Med. 2011 Oct 20;365(16):1538-40. doi: 10.1056/NEJMe1109546. N Engl J Med. 2011. PMID: 22010921 No abstract available.
-
Timing of antiretroviral therapy for HIV-1-associated tuberculosis.N Engl J Med. 2012 Feb 2;366(5):474; author reply 475-6. doi: 10.1056/NEJMc1113986. N Engl J Med. 2012. PMID: 22296084 No abstract available.
-
ACP Journal Club. Earlier initiation of antiretroviral therapy after start of antituberculosis therapy reduced mortality in HIV.Ann Intern Med. 2012 Mar 20;156(6):JC3-2. doi: 10.7326/0003-4819-156-6-201203200-02002. Ann Intern Med. 2012. PMID: 22431688 No abstract available.
References
-
- Global tuberculosis control: WHO report 2010. Geneva: World Health Organization; 2010.
-
- Mukadi YD, Maher D, Harries A. Tuberculosis case fatality rates in high HIV prevalence populations in sub-Saharan Africa. AIDS. 2001;15:143–52. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials