

Transplantation outcomes in primary hyperoxaluria
- PMID: 20849551
- PMCID: PMC2965313
- DOI: 10.1111/j.1600-6143.2010.03271.x
Transplantation outcomes in primary hyperoxaluria
Abstract
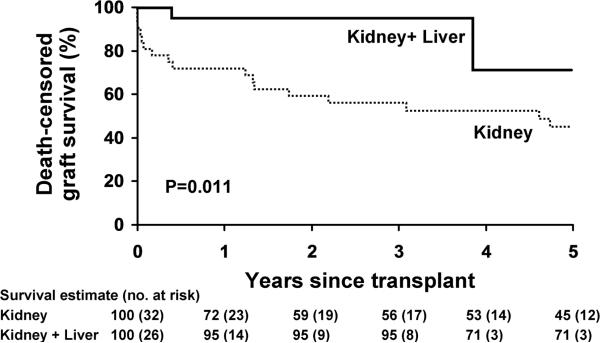
Optimal transplantation strategies are uncertain in primary hyperoxaluria (PH) due to potential for recurrent oxalosis. Outcomes of different transplantation approaches were compared using life-table methods to determine kidney graft survival among 203 patients in the International Primary Hyperoxaluria Registry. From 1976-2009, 84 kidney alone (K) and combined kidney and liver (K + L) transplants were performed in 58 patients. Among 58 first kidney transplants (32 K, 26 K + L), 1-, 3- and 5-year kidney graft survival was 82%, 68% and 49%. Renal graft loss occurred in 26 first transplants due to oxalosis in ten, chronic allograft nephropathy in six, rejection in five and other causes in five. Delay in PH diagnosis until after transplant favored early graft loss (p = 0.07). K + L had better kidney graft outcomes than K with death-censored graft survival 95% versus 56% at 3 years (p = 0.011). Among 29 year 2000-09 first transplants (24 K + L), 84% were functioning at 3 years compared to 55% of earlier transplants (p = 0.05). At 6.8 years after transplantation, 46 of 58 patients are living (43 with functioning grafts). Outcomes of transplantation in PH have improved over time, with recent K + L transplantation highly successful. Recurrent oxalosis accounted for a minority of kidney graft losses.
©2010 The Authors Journal compilation©2010 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures







References
-
- Danpure CJ, Jennings PR. Peroxisomal alanine:glyoxylate aminotransferase deficiency in primary hyperoxaluria type 1. FEBS letter. 1986;201:20–24. - PubMed
-
- Mistry J, Danpure CJ, Chalmers RA. Hepatic D-glycerate dehydrogenase and glyoxylate reductase deficiency in primary hyperoxaluria type 2. Biochem Soc Trans. 1988;16:626–627.
-
- Vervaet BA, Verhulst A, D'Haese PC, De Broe ME. Nephrocalcinosis: new insights into mechanisms and consequences. Nephrol Dial Transplant. 2009;24:2030–2035. - PubMed
-
- Leumann E, Hoppe B. The primary hyperoxalurias. J Am Soc Nephrol. 2001;12:1986–1993. - PubMed
-
- Milliner DS, Eickholt JT, Bergstralh E, Wilson DM, Smith LH. Primary hyperoxaluria: Results of long-term treatment with orthophosphate and pyridoxine. New Engl J Med. 1994;331:1553–1558. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
