

Impact of Point-of-Care Birth Test-and-Treat on Clinical Outcomes Among Infants With HIV: A Cluster-Randomized Trial in Mozambique and Tanzania
- PMID: 39514367
- PMCID: PMC12135909
- DOI: 10.1093/cid/ciae530
Impact of Point-of-Care Birth Test-and-Treat on Clinical Outcomes Among Infants With HIV: A Cluster-Randomized Trial in Mozambique and Tanzania
Abstract
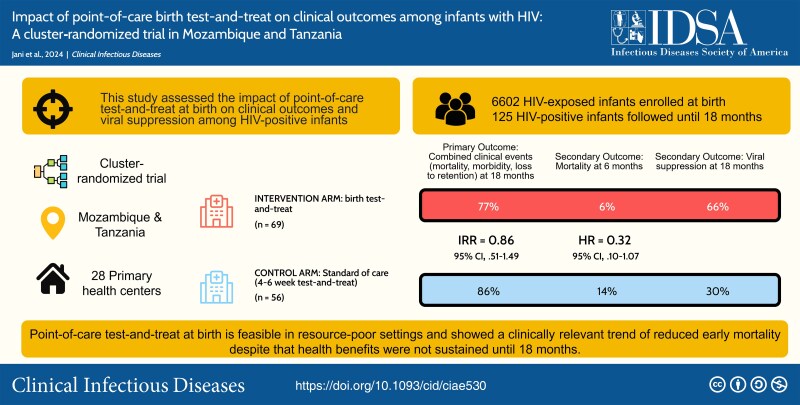
Background: We assessed the impact of point-of-care (PoC) test-and-treat at birth on clinical outcomes and viral suppression among human immunodeficiency virus (HIV)-positive infants in Mozambique and Tanzania.
Methods: This cluster-randomized trial allocated health facilities to intervention, providing PoC testing and antiretroviral treatment (ART) at birth and week 4-8, or control, starting these at week 4-8. The primary outcome was proportions of clinical events (mortality, morbidity, retention, virological failure, toxicity) among HIV-positive infants at month 18. We estimated incidence rate ratios adjusted for timing of HIV detection (aIRR) and reported viral suppression <1000 copies/mL.
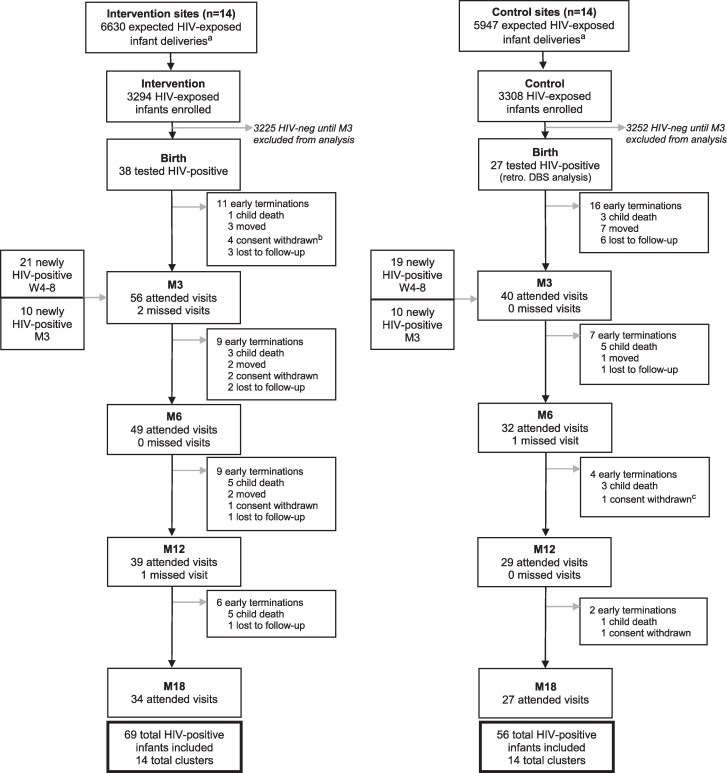
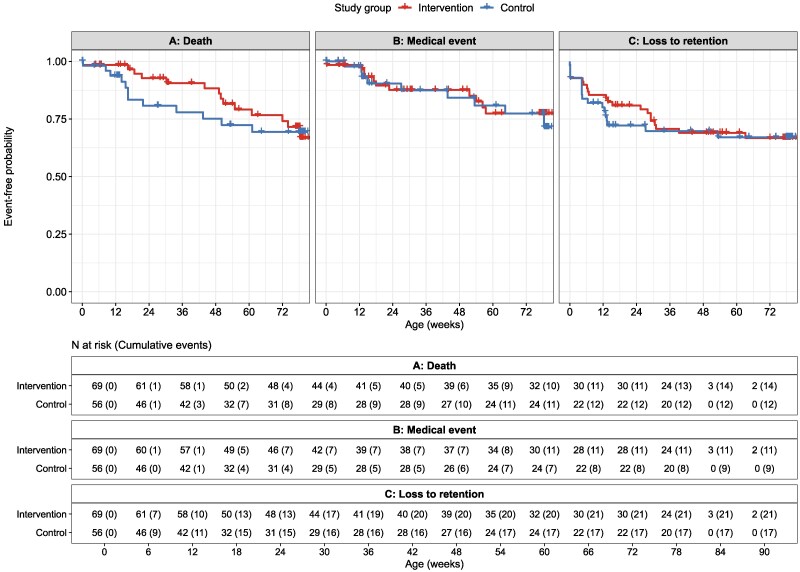
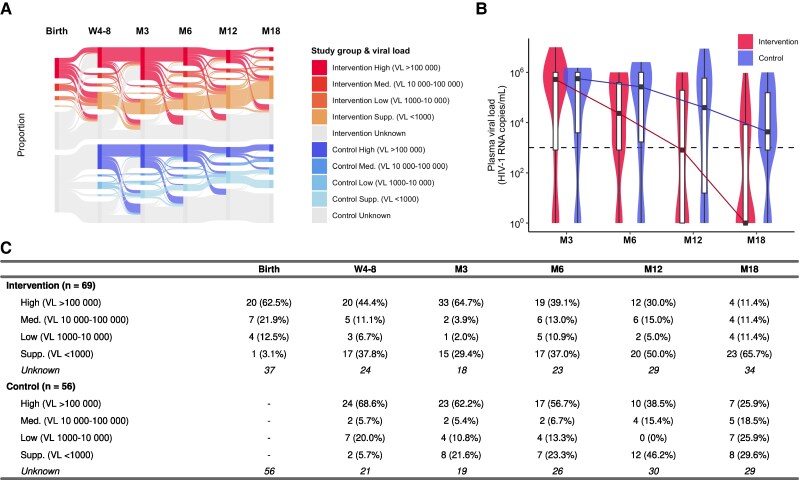
Results: Among 6602 neonates enrolled during October 2019-September 2021, 125 were diagnosed with HIV by week 12. In the intervention arm, 38 of 69 (55.1%) were diagnosed at birth. In the control arm, 27 of 56 (48.2%) were retrospectively detected to be HIV-positive at birth, of whom 6 of 56 (10.7%) died or were lost to follow-up before testing. Median age at ART initiation was 6 (intervention) versus 33 days (control). Birth test-and-treat was not associated with a significant reduction in clinical outcomes up to month 18 (53 [76.8%] vs 48 [85.7%]; aIRR, 0.857 [95% confidence interval, .505-1.492]), but showed a 68% relative reduction in 6-month mortality. Viral suppression was poor overall.
Conclusions: PoC test-and-treat at birth is feasible in resource-poor settings and resulted in clinically relevant reduction of early mortality, though improved clinical outcomes were not sustained to month 18. Poor viral suppression may undermine early benefits, calling for better pediatric treatments and adherence interventions. Clinical Trials Registration. NCT04032522.
Keywords: HIV; birth testing; neonatal treatment; point-of-care testing; test-and-treat.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Figures
References
-
- Joint United Nations Programme on HIV/AIDS . UNAIDS data 2023. UNAIDS data 2023. 2023. Available at: https://www.unaids.org/en/resources/documents/2023/2023_unaids_data. Accessed 1 August 2024.
-
- Newell ML, Coovadia H, Cortina-Borja M, et al. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet 2004; 364:1236–43. - PubMed
-
- Bourne DE, Thompson M, Brody LL, et al. Emergence of a peak in early infant mortality due to HIV/AIDS in South Africa. AIDS 2009; 23:101–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
