

Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial
- PMID: 21062666
- PMCID: PMC3033534
- DOI: 10.1016/S0140-6736(10)61924-1
Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial
Erratum in
- Lancet. 2011 Jan 8;377(9760):126
Abstract
Background: Severe malaria is a major cause of childhood death and often the main reason for paediatric hospital admission in sub-Saharan Africa. Quinine is still the established treatment of choice, although evidence from Asia suggests that artesunate is associated with a lower mortality. We compared parenteral treatment with either artesunate or quinine in African children with severe malaria.
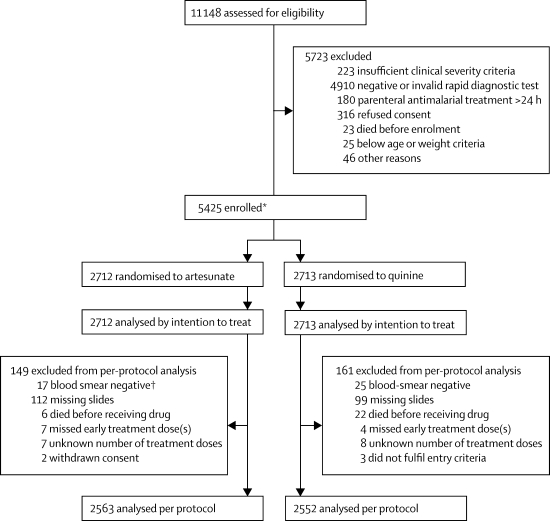
Methods: This open-label, randomised trial was undertaken in 11 centres in nine African countries. Children (<15 years) with severe falciparum malaria were randomly assigned to parenteral artesunate or parenteral quinine. Randomisation was in blocks of 20, with study numbers corresponding to treatment allocations kept inside opaque sealed paper envelopes. The trial was open label at each site, and none of the investigators or trialists, apart from for the trial statistician, had access to the summaries of treatment allocations. The primary outcome measure was in-hospital mortality, analysed by intention to treat. This trial is registered, number ISRCTN50258054.
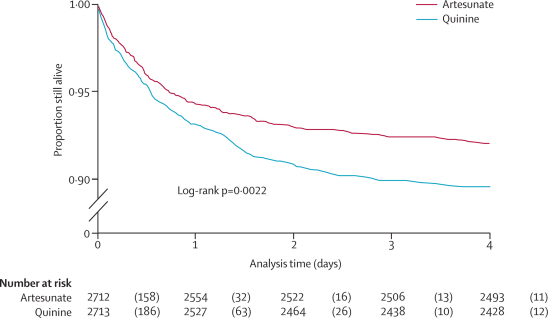
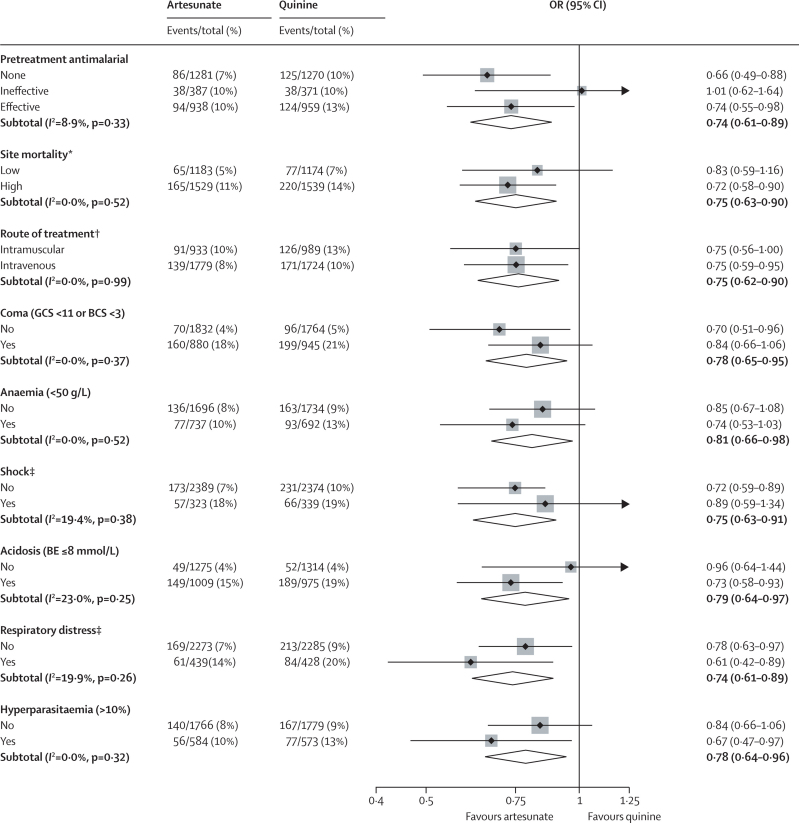
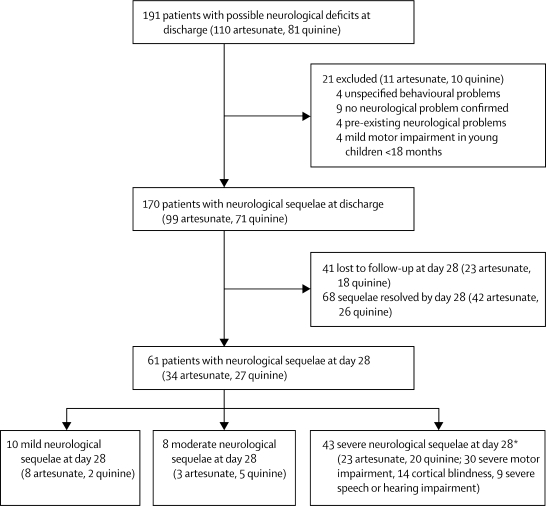
Findings: 5425 children were enrolled; 2712 were assigned to artesunate and 2713 to quinine. All patients were analysed for the primary outcome. 230 (8·5%) patients assigned to artesunate treatment died compared with 297 (10·9%) assigned to quinine treatment (odds ratio [OR] stratified for study site 0·75, 95% CI 0·63-0·90; relative reduction 22·5%, 95% CI 8·1-36·9; p=0·0022). Incidence of neurological sequelae did not differ significantly between groups, but the development of coma (65/1832 [3·5%] with artesunate vs 91/1768 [5·1%] with quinine; OR 0·69 95% CI 0·49-0·95; p=0·0231), convulsions (224/2712 [8·3%] vs 273/2713 [10·1%]; OR 0·80, 0·66-0·97; p=0·0199), and deterioration of the coma score (166/2712 [6·1%] vs 208/2713 [7·7%]; OR 0·78, 0·64-0·97; p=0·0245) were all significantly less frequent in artesunate recipients than in quinine recipients. Post-treatment hypoglycaemia was also less frequent in patients assigned to artesunate than in those assigned to quinine (48/2712 [1·8%] vs 75/2713 [2·8%]; OR 0·63, 0·43-0·91; p=0·0134). Artesunate was well tolerated, with no serious drug-related adverse effects.
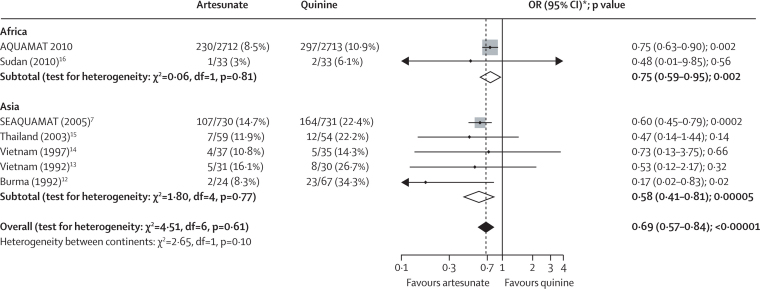
Interpretation: Artesunate substantially reduces mortality in African children with severe malaria. These data, together with a meta-analysis of all trials comparing artesunate and quinine, strongly suggest that parenteral artesunate should replace quinine as the treatment of choice for severe falciparum malaria worldwide.
Funding: The Wellcome Trust.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
For severe malaria, artesunate is the answer.Lancet. 2010 Nov 13;376(9753):1621-2. doi: 10.1016/S0140-6736(10)61928-9. Epub 2010 Nov 7. Lancet. 2010. PMID: 21062665 No abstract available.
-
Artesunate for severe malaria in African children.Lancet. 2011 Apr 2;377(9772):1153-4; author reply 1154. doi: 10.1016/S0140-6736(11)60463-7. Lancet. 2011. PMID: 21459208 No abstract available.
References
-
- WHO Severe and complicated malaria. Trans R Soc Trop Med Hyg. 1990;84(suppl 2):1–65. - PubMed
-
- WHO Severe and complicated malaria. Trans R Soc Trop Med Hyg. 2000;94(suppl 1):1–90. - PubMed
-
- White NJ. The treatment of malaria. N Engl J Med. 1996;335:800–806. - PubMed
-
- Yen LM, Dao LM, Day NP. Role of quinine in the high mortality of intramuscular injection tetanus. Lancet. 1994;344:786–877. - PubMed
-
- White NJ, Warrell DA, Chanthavanich P. Severe hypoglycemia and hyperinsulinemia in falciparum malaria. N Engl J Med. 1983;309:61–66. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
