

Exposing and Overcoming Limitations of Clinical Laboratory Tests in COVID-19 by Adding Immunological Parameters; A Retrospective Cohort Analysis and Pilot Study
- PMID: 35844497
- PMCID: PMC9276968
- DOI: 10.3389/fimmu.2022.902837
Exposing and Overcoming Limitations of Clinical Laboratory Tests in COVID-19 by Adding Immunological Parameters; A Retrospective Cohort Analysis and Pilot Study
Abstract
Background: Two years since the onset of the COVID-19 pandemic no predictive algorithm has been generally adopted for clinical management and in most algorithms the contribution of laboratory variables is limited.
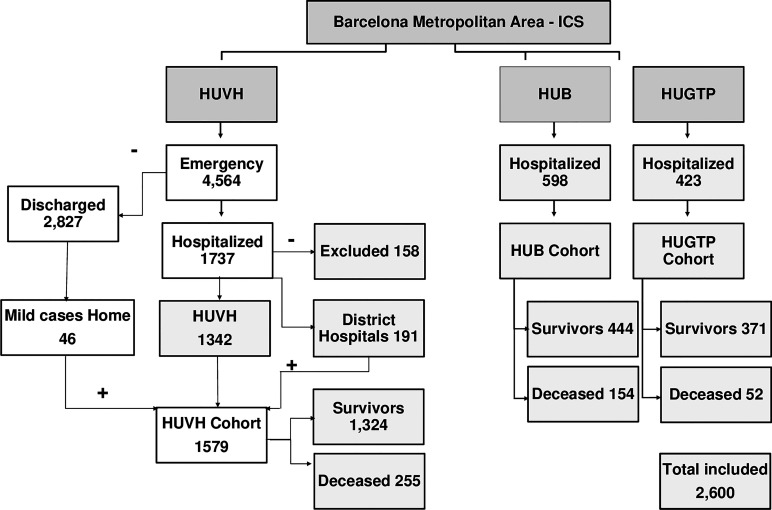
Objectives: To measure the predictive performance of currently used clinical laboratory tests alone or combined with clinical variables and explore the predictive power of immunological tests adequate for clinical laboratories. Methods: Data from 2,600 COVID-19 patients of the first wave of the pandemic in the Barcelona area (exploratory cohort of 1,579, validation cohorts of 598 and 423 patients) including clinical parameters and laboratory tests were retrospectively collected. 28-day survival and maximal severity were the main outcomes considered in the multiparametric classical and machine learning statistical analysis. A pilot study was conducted in two subgroups (n=74 and n=41) measuring 17 cytokines and 27 lymphocyte phenotypes respectively.
Findings: 1) Despite a strong association of clinical and laboratory variables with the outcomes in classical pairwise analysis, the contribution of laboratory tests to the combined prediction power was limited by redundancy. Laboratory variables reflected only two types of processes: inflammation and organ damage but none reflected the immune response, one major determinant of prognosis. 2) Eight of the thirty variables: age, comorbidity index, oxygen saturation to fraction of inspired oxygen ratio, neutrophil-lymphocyte ratio, C-reactive protein, aspartate aminotransferase/alanine aminotransferase ratio, fibrinogen, and glomerular filtration rate captured most of the combined statistical predictive power. 3) The interpretation of clinical and laboratory variables was moderately improved by grouping them in two categories i.e., inflammation related biomarkers and organ damage related biomarkers; Age and organ damage-related biomarker tests were the best predictors of survival, and inflammatory-related ones were the best predictors of severity. 4) The pilot study identified immunological tests (CXCL10, IL-6, IL-1RA and CCL2), that performed better than most currently used laboratory tests.
Conclusions: Laboratory tests for clinical management of COVID 19 patients are valuable but limited predictors due to redundancy; this limitation could be overcome by adding immunological tests with independent predictive power. Understanding the limitations of tests in use would improve their interpretation and simplify clinical management but a systematic search for better immunological biomarkers is urgent and feasible.
Keywords: CXCL10; SARS-CoV-2 infection; acute phase reactants; chemokines; clinical laboratory tests; cytokines; flow cytometry; predictive risk-profile.
Copyright © 2022 Sánchez-Montalvá, Álvarez-Sierra, Martínez-Gallo, Perurena-Prieto, Arrese-Muñoz, Ruiz-Rodríguez, Espinosa-Pereiro, Bosch-Nicolau, Martínez-Gómez, Antón, Martínez-Valle, Riveiro-Barciela, Blanco-Grau, Rodríguez-Frias, Castellano-Escuder, Poyatos-Canton, Bas-Minguet, Martínez-Cáceres, Sánchez-Pla, Zurera-Egea, Teniente-Serra, Hernández-González, Pujol-Borrell and the “Hospital Vall d’Hebron Group for the study of COVID-19 immune profile”.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures







References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous