

Population-based rates, risk factors and consequences of preterm births in South-Asia and sub-Saharan Africa: A multi-country prospective cohort study
- PMID: 35198148
- PMCID: PMC8850944
- DOI: 10.7189/jogh.12.04011
Population-based rates, risk factors and consequences of preterm births in South-Asia and sub-Saharan Africa: A multi-country prospective cohort study
Abstract
Background: Preterm birth is the leading cause of neonatal deaths in low middle-income countries (LMICs), yet there exists a paucity of high-quality data from these countries. Most modelling estimates are based on studies using inaccurate methods of gestational age assessment. We aimed to fill this gap by measuring the population-based burden of preterm birth using early ultrasound dating in five countries in South-Asian and sub-Saharan Africa.
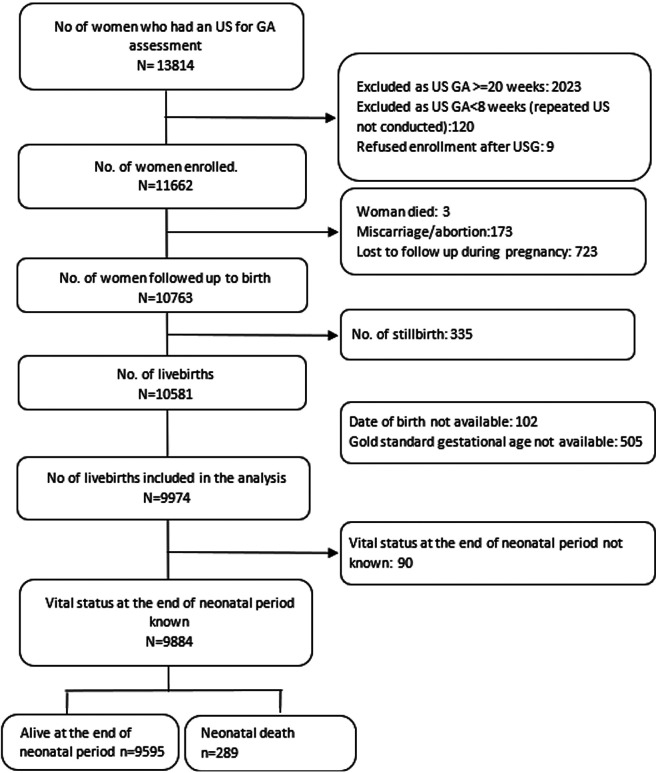
Methods: We identified women early in pregnancy (<20 weeks based on last menstrual period) by home visits every 2-3 months (except in Zambia where they were identified at antenatal care clinics) in 5 research sites in South-Asia and sub-Saharan Africa between July 2012 and September 2016. Trained sonographers performed an ultrasound scan for gestational age dating. Women were enrolled if they were 8-19 weeks pregnant on ultrasound. Women <8 weeks were rescheduled for repeat scans after 4 weeks, and identified women were followed through pregnancy until 6 weeks postpartum. Site-specific rates and proportions were calculated and a logistic regression model was used to predict the risk factors of preterm birth.
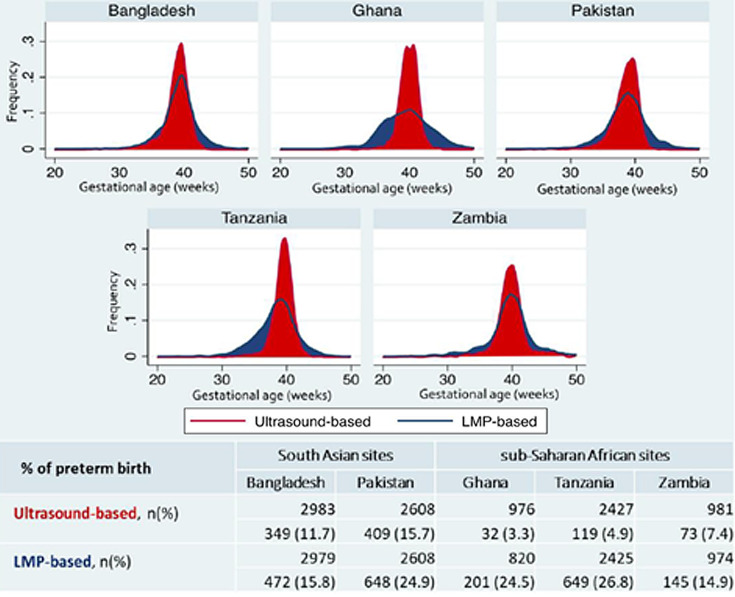
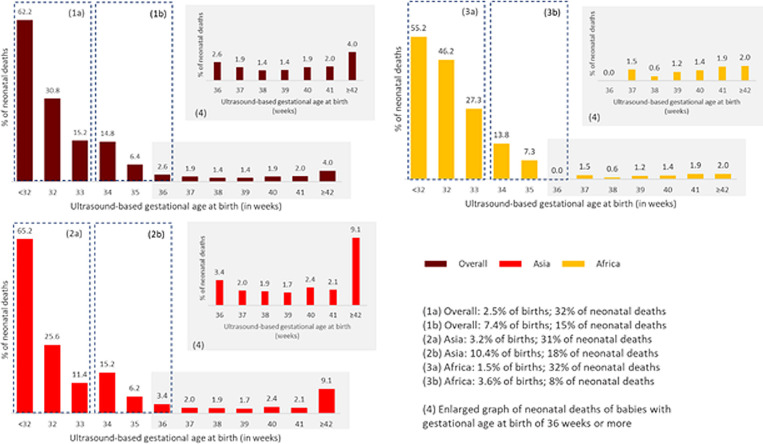
Results: Preterm birth rates ranged from 3.2% in Ghana to 15.7% in Pakistan. About 46% of all neonatal deaths occurred among preterm infants, 49% in South Asia and 40% in sub-Saharan Africa. Fourteen percent of all preterm infants died during the neonatal period. The mortality was 37.6% for early preterm babies (<34 weeks), 5.9% for late preterm babies (34 to <37 weeks), and 1.7% for term babies (37 to <42 weeks). Factors associated lower gestation at birth included South-Asian region (adjusted mean difference (Adj MD) = -6.2 days, 95% confidence interval (CI) = -5.5, -6.9), maternal morbidities (Adj MD = -3.4 days, 95% CI = -4.6, -2.2), multiple pregnancies (Adj MD = -17.8 days, 95% CI = -19.9,-15.8), adolescent pregnancy (Adj MD = -2.7 days, 95% CI = -3.7, -1.6) and lowest wealth quintile (Adj MD = -1.3 days, 95% CI = -2.4, -0.3).
Conclusions: Preterm birth rates are higher in South Asia than in sub-Saharan Africa and contribute to 49% and 40% of all neonatal deaths in the two regions, respectively. Adolescent pregnancy and maternal morbidities are modifiable risk factors associated with preterm birth.
Copyright © 2022 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Competing interests: The WHO and study sites received funding from the Bill and Melinda Gates Foundation (BMGF) to conduct this study. BB, CBA, DHH, JH, LH, FM, KES, MSS and JW report research grants from the BMGF during the conduct of the study. ACL reported research grants from the NICHD and BMGF. The authors completed the ICMJE Declaration of Interest form (available upon request from the corresponding authors), and declare no further conflicts of interest.
Figures
References
-
- WHO recommended definitions, terminology and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths. Modifications recommended by FIGO as amended October 14, 1976. Acta Obstet Gynecol Scand. 1977;56:247-53. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
