

Effectiveness and safety of integrase strand transfer inhibitors in Spain: a prospective real-world study
- PMID: 37434782
- PMCID: PMC10331300
- DOI: 10.3389/fcimb.2023.1187999
Effectiveness and safety of integrase strand transfer inhibitors in Spain: a prospective real-world study
Abstract
Introduction: Second-generation integrase strand transfer inhibitors (INSTIs) are preferred treatment options worldwide, and dolutegravir (DTG) is the treatment of choice in resource-limited settings. Nevertheless, in some resource-limited settings, these drugs are not always available. An analysis of the experience with the use of INSTIs in unselected adults living with HIV may be of help to make therapeutic decisions when second-generation INSTIs are not available. This study aimed to evaluate the real-life effectiveness and safety of dolutegravir (DTG), elvitegravir/cobicistat (EVG/c), and raltegravir (RAL) in a large Spanish cohort of HIV-1-infected patients.
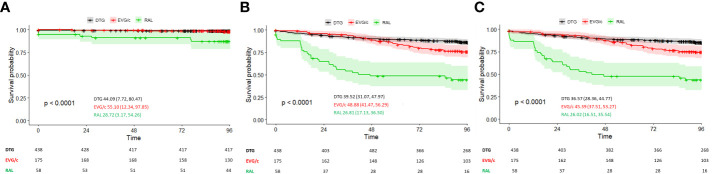
Methods: Real-world study of adults living with HIV who initiated integrase INSTIs DTG, EVG/c, and RAL-based regimens in three settings (ART-naïve patients, ART-switching, and ART-salvage patients). The primary endpoint was the median time to treatment discontinuation after INSTI-based regimen initiation. Proportion of patients experiencing virological failure (VF) (defined as two consecutive viral loads (VL) ≥200 copies/mL at 24 weeks or as a single determination of VL ≥1,000 copies/mL while receiving DTG, EVG/c or RAL, and at least 3 months after INSTI initiation) and time to VF were also evaluated.
Results: Virological effectiveness of EVG/c- and RAL-based regimens was similar to that of DTG when given as first-line and salvage therapy. Treatment switching for reasons other than virological failure was more frequent in subjects receiving EVG/c and, in particular, RAL. Naïve patients with CD4+ nadir <100 cells/μL were more likely to develop VF, particularly if they initiated RAL or EVG/c. In the ART switching population, initiation of RAL and EVG/c was associated with both VF and INSTI discontinuation. There were no differences in the time to VF and INSTI discontinuation between DTG, EVG/c and RAL. Immunological parameters improved in the three groups and for the three drugs assessed. Safety and tolerability were consistent with expected safety profiles.
Discussion: Whereas second-generation INSTIs are preferred treatment options worldwide, and DTG is one of the treatment of choices in resource-limited settings, first-generation INSTIs may still provide high virological and immunological effectiveness when DTG is not available.
Keywords: HIV; dolutegravir; elvitegravir; integrase strand transfer inhibitors (INSTI); raltegravir; real-world study.
Copyright © 2023 Santos, Casadellà, Noguera-Julian, Micán-Rivera, Domingo, Antela, Portilla, Sanz, Montero-Alonso, Navarro, Masiá, Valcarce-Pardeiro, Ocampo, Pérez-Martínez, García-Vallecillos, Vivancos, Imaz, Iribarren, Hernández-Quero, Villar-García, Barrufet, Paredes and INSTINCT study group.
Conflict of interest statement
JRS, AA, AO, and JP have received research funding, consultancy fees and lecture sponsorships from, and have served on advisory boards for Gilead Sciences, Janssen-Cilag, Merck Sharp & Dohme and ViiV Healthcare. JP and JS have received research funding and consultancy fees from, and have served on advisory boards for Gilead Sciences, Merck Sharp & Dohme and ViiV Healthcare. PD has received honoraria for speaking or participating in advisory boards and/or research grants from the following pharmaceutical companies: Glaxo SmithKline GSK, Abbvie, Boehringer-Ingelheim, Bristol-Myers Squibb, Jansen & Cilag, Merck & Dohme, Gilead Sciences, Pfizer Inc, Thera technologies, ViiV Healthcare, Roche, and Ferrer International. MM has received research funding, consultancy fees and lecture sponsorships from, and has served on advisory boards for Janssen-Cilag, Merck Sharp & Dohme and ViiV Healthcare. MM-A has received consultancy fees and lecture sponsorships from and has served on advisory boards for Gilead Sciences, Janssen-Cilag, ViiV Healthcare and Merck Sharp & Dohme. JN has received fees for educational activities and/or consultancies and/or financial support for attending conferences from Abbvie, Gilead Science, Janssen-Cilag, Merck Sharp & Dohme and ViiV Healthcare out of the submitted work. MV has received research funding, consultancy fees and lecture sponsorships from, and has served on advisory boards for Gilead and ViiV Healthcare. AI has received research funding, consultancy fees, and lecture sponsorships from, or has served on advisory boards for Gilead Sciences, Janssen-Cilag, Merck Sharp & Dohme, Thera Technologies and ViiV Healthcare. PB has received consultancy fees from, and has served on advisory boards for Gilead Sciences, Merck Sharp & Dohme, Janssen-Cilag and ViiV Healthcare. RP has received research funding and consultancy fees and/or has served on advisory boards for Boehringer-Ingelheim, Gilead Sciences, Glaxo Smith-Kline, Merck Sharp & Dohme, Pfizer, and ViiV Healthcare. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Abram M. E., Hluhanich R. M., Goodman D. D., Andreatta K. N., Margot N. A., Ye L., et al. . (2013). Impact of primary elvitegravir resistance-associated mutations in HIV-1 integrase on drug susceptibility and viral replication fitness. Antimicrob. Agents Chemother. 57 (6), 2654–2663. doi: 10.1128/AAC.02568-12 - DOI - PMC - PubMed
-
- Bill and Melinda Gates Foundation (2020). HIV MARKET REPORT the state of HIV treatment, testing, and prevention in low- and middle-income countries. (383 Dorchester Avenue, Suite 400, Boston, MA 02127 USA: Clinton Health Access Initiative, Inc.) 11, 1–30.
-
- Brehm T. T., Franz M., Hüfner A., Hertling S., Schmiedel S., Degen O., et al. . (2019). Safety and efficacy of elvitegravir, dolutegravir, and raltegravir in a real-world cohort of treatment-naïve and -experienced patients. Med. (United States) 98 (32), 1–7. doi: 10.1097/MD.0000000000016721 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials