

Clinical implementation of preemptive pharmacogenomics in psychiatry
- PMID: 38364700
- PMCID: PMC10879811
- DOI: 10.1016/j.ebiom.2024.105009
Clinical implementation of preemptive pharmacogenomics in psychiatry
Abstract
Background: Pharmacogenomics (PGx) holds promise to revolutionize modern healthcare. Although there are several prospective clinical studies in oncology and cardiology, demonstrating a beneficial effect of PGx-guided treatment in reducing adverse drug reactions, there are very few such studies in psychiatry, none of which spans across all main psychiatric indications, namely schizophrenia, major depressive disorder and bipolar disorder. In this study we aim to investigate the clinical effectiveness of PGx-guided treatment (occurrence of adverse drug reactions, hospitalisations and re-admissions, polypharmacy) and perform a cost analysis of the intervention.
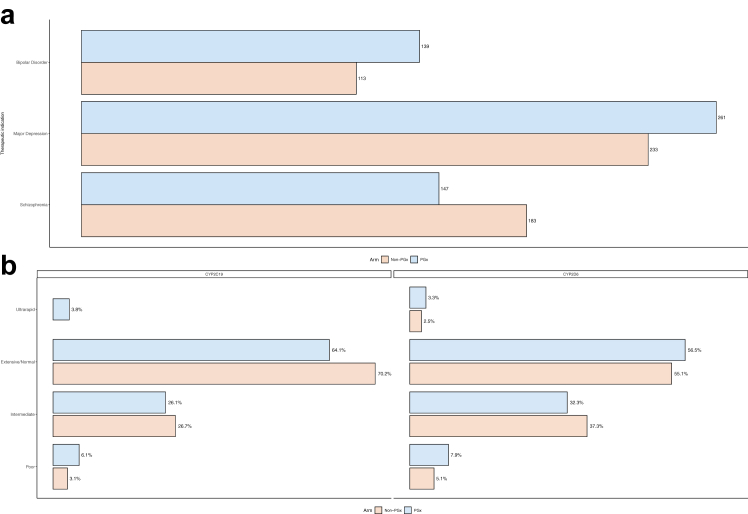
Methods: We report our findings from a multicenter, large-scale, prospective study of pre-emptive genome-guided treatment named as PREemptive Pharmacogenomic testing for preventing Adverse drug REactions (PREPARE) in a large cohort of psychiatric patients (n = 1076) suffering from schizophrenia, major depressive disorder and bipolar disorder.
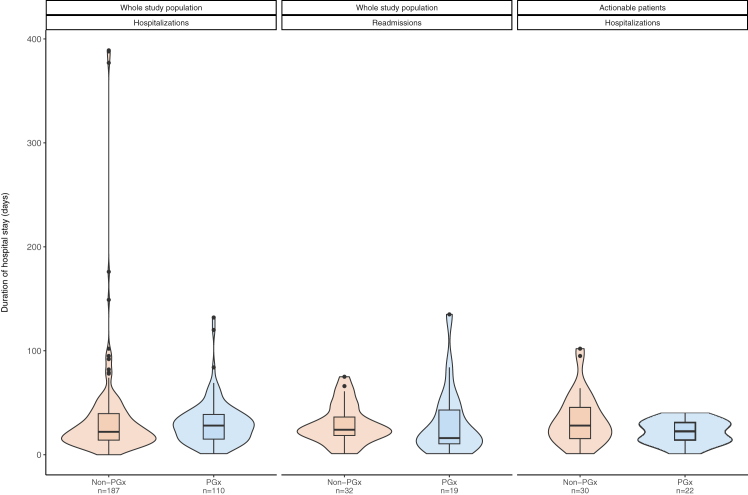
Findings: We show that patients with an actionable phenotype belonging to the PGx-guided arm (n = 25) present with 34.1% less adverse drug reactions compared to patients belonging to the control arm (n = 36), 41.2% less hospitalisations (n = 110 in the PGx-guided arm versus n = 187 in the control arm) and 40.5% less re-admissions (n = 19 in the PGx-guided arm versus n = 32 in the control arm), less duration of initial hospitalisations (n = 3305 total days of hospitalisation in the PGx-guided arm from 110 patients, versus n = 6517 in the control arm from 187 patients) and duration of hospitalisation upon readmission (n = 579 total days of hospitalisation upon readmission in the PGx-guided arm, derived from 19 patients, versus n = 928 in the control arm, from 32 patients respectively). It was also shown that in the vast majority of the cases, there was less drug dose administrated per drug in the PGx-guided arm compared to the control arm and less polypharmacy (n = 124 patients prescribed with at least 4 psychiatric drugs in the PGx-guided arm versus n = 143 in the control arm) and smaller average number of co-administered psychiatric drugs (2.19 in the PGx-guided arm versus 2.48 in the control arm. Furthermore, less deaths were reported in the PGx-guided arm (n = 1) compared with the control arm (n = 9). Most importantly, we observed a 48.5% reduction of treatment costs in the PGx-guided arm with a reciprocal slight increase of the quality of life of patients suffering from major depressive disorder (0.935 versus 0.925 QALYs in the PGx-guided and control arm, respectively).
Interpretation: While only a small proportion (∼25%) of the entire study sample had an actionable genotype, PGx-guided treatment can have a beneficial effect in psychiatric patients with a reciprocal reduction of treatment costs. Although some of these findings did not remain significant when all patients were considered, our data indicate that genome-guided psychiatric treatment may be successfully integrated in mainstream healthcare.
Funding: European Union Horizon 2020.
Keywords: Bipolar disorder; Clinical implementation; Cost-effectiveness; Major depressive disorder; Preemptive pharmacogenomics; Schizophrenia.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
References
-
- Squassina A., Manchia M., Manolopoulos V.G., et al. Realities and expectations of pharmacogenomics and personalized medicine: impact of translating genetic knowledge into clinical practice. Pharmacogenomics. 2010;11(8):1149–1167. - PubMed
-
- van der Wouden C.H., Cambon-Thomsen A., Cecchin E., et al. Implementing pharmacogenomics in Europe: design and implementation strategy of the ubiquitous pharmacogenomics consortium. Clin Pharmacol Ther. 2017;101(3):341–358. - PubMed
-
- Swen J.J., van der Wouden C.H., Manson L.E., et al. A 12-gene pharmacogenetic panel to prevent adverse drug reactions: an open-label, multicentre, controlled, cluster-randomised crossover implementation study. Lancet. 2023;401(10374):347–356. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
