

Quantitative detection of immune activation transcripts as a diagnostic tool in kidney transplantation
- PMID: 9012847
- PMCID: PMC19576
- DOI: 10.1073/pnas.94.2.695
Quantitative detection of immune activation transcripts as a diagnostic tool in kidney transplantation
Abstract
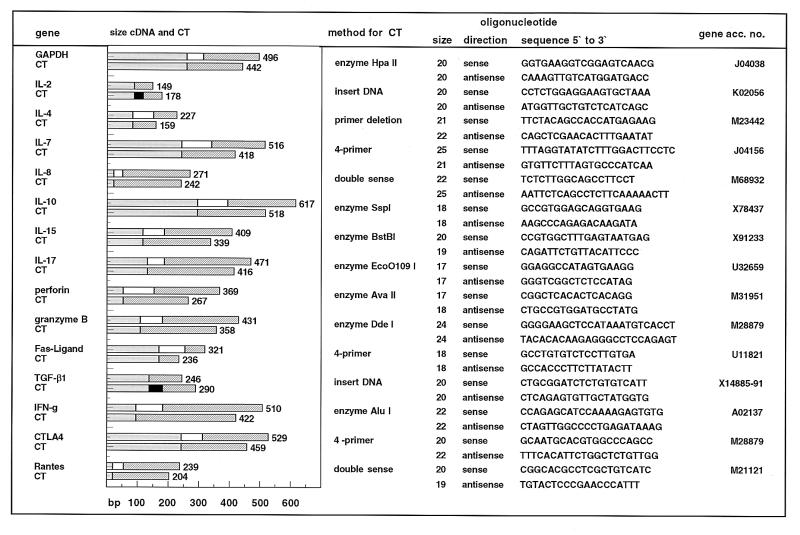
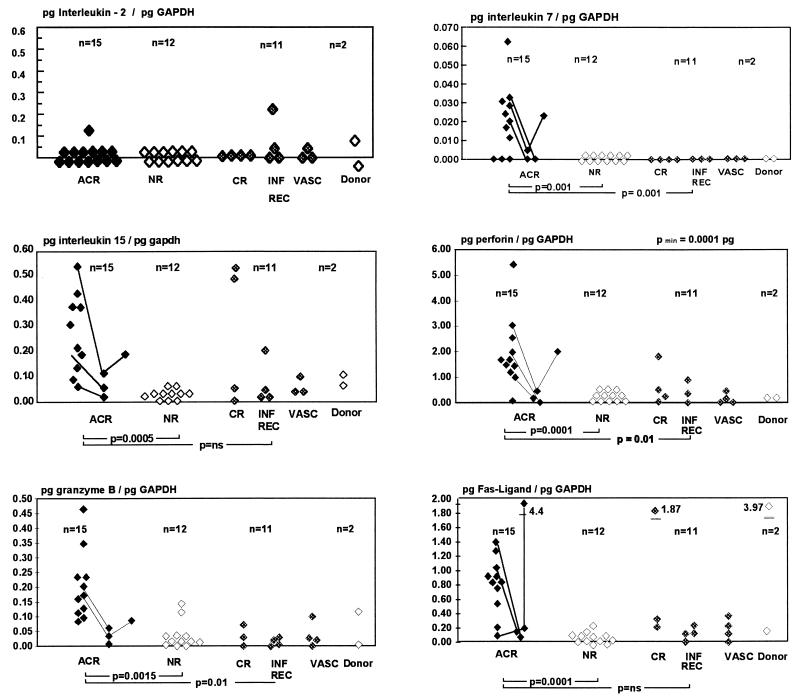
Procedures to diagnose renal allograft rejection depend upon detection of graft dysfunction and the presence of a mononuclear leukocytic infiltrate; however, the presence of a modest cellular infiltrate is often not conclusive and can be detected in non-rejecting grafts. We have pursued a molecular approach utilizing reverse transcription (RT)-PCR to test the diagnostic accuracy of multiple immune activation gene analysis as means to diagnose renal allograft rejection. The magnitude of intragraft gene expression of 15 immune activation genes was quantified by competitive RT-PCR in 60 renal allograft core biopsies obtained for surveillance or to diagnose the etiology of graft dysfunction. Results were compared with a clinicopathological analysis based upon the histological diagnosis (Banff criteria) and the response to antirejection treatment. During acute renal allograft rejection intragraft expression of the interleukin (IL)-7 (P < 0.001), IL-10 (P < 0.0001), IL-15 (P < 0.0001), Fas ligand (P < 0.0001), perforin (P < 0.0001), and granzyme B (P < 0.0015), but not IL-2, interferon gamma, or IL-4, genes is significantly heightened. Amplified RANTES and IL-8 gene transcripts are sensitive but nonspecific markers of rejection. A simultaneous RT-PCR evaluation of perforin, granzyme B, and Fas ligand identifies acute rejection, including cases with mild infiltration, with extraordinary sensitivity (100%) and specificity (100%). Effective antirejection therapy results in a rapid down-regulation of gene expression. The combined analysis of Fas ligand, perforin, and granzyme B gene expression by quantitative RT-PCR provides a reliable tool for diagnosis and follow-up of acute renal allograft rejection. Its accuracy and a potential rapid application within few hours suggest its use in the clinical management of renal transplant patients.
Figures
References
-
- Cecka, J. M. & Terasaki, P. I. (1993) Clin. Transplant. 1993, 1–18. - PubMed
-
- Tejani A, Stablein D, Alexander S, Fine R, Harmon W. Transplantation. 1995;59:500–504. - PubMed
-
- Solez K, Axelsen R A, Benediktsson H, Burdick J F, Cohen A H, Colvin R B, Croker R P, Droz D, Dunik M S, Halloran P F. Kidney Int. 1993;44:411–422. - PubMed
-
- Rush D N, Henry S F, Jeffery J R, Schroeder T J, Gough J. Transplantation. 1994;57:208–211. - PubMed
-
- Rush D N, Jeffrey J R, Gough J. Transplantation. 1994;59:511–514. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
