

Combination Therapy with Oral Treprostinil for Pulmonary Arterial Hypertension. A Double-Blind Placebo-controlled Clinical Trial
- PMID: 31765604
- PMCID: PMC7068822
- DOI: 10.1164/rccm.201908-1640OC
Combination Therapy with Oral Treprostinil for Pulmonary Arterial Hypertension. A Double-Blind Placebo-controlled Clinical Trial
Abstract
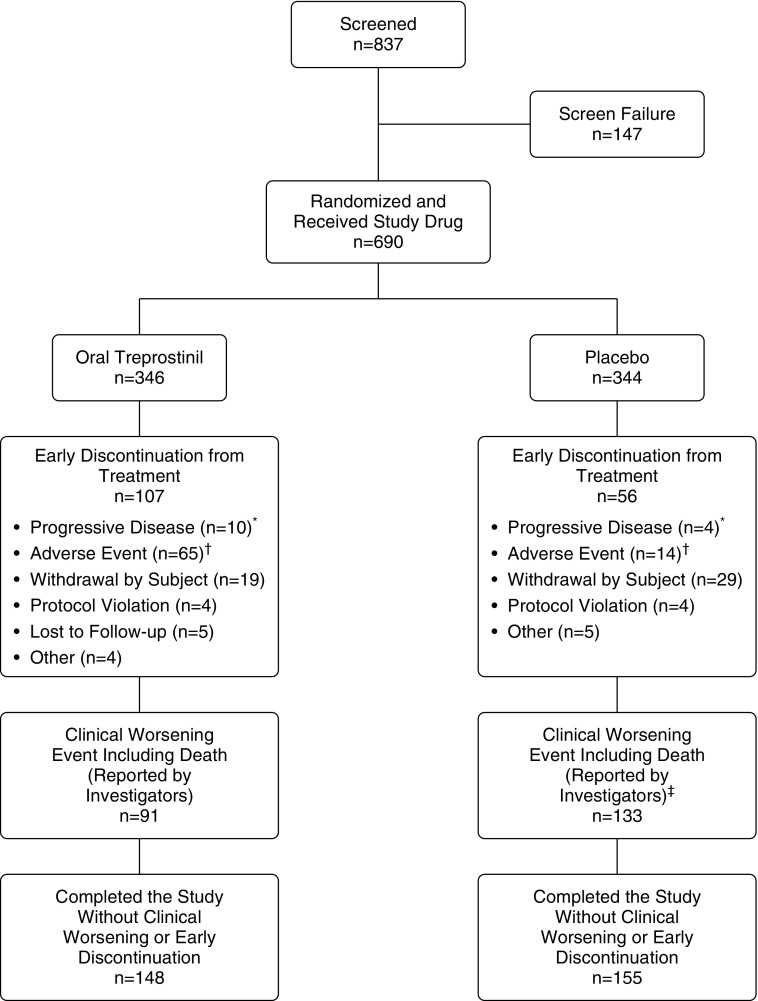
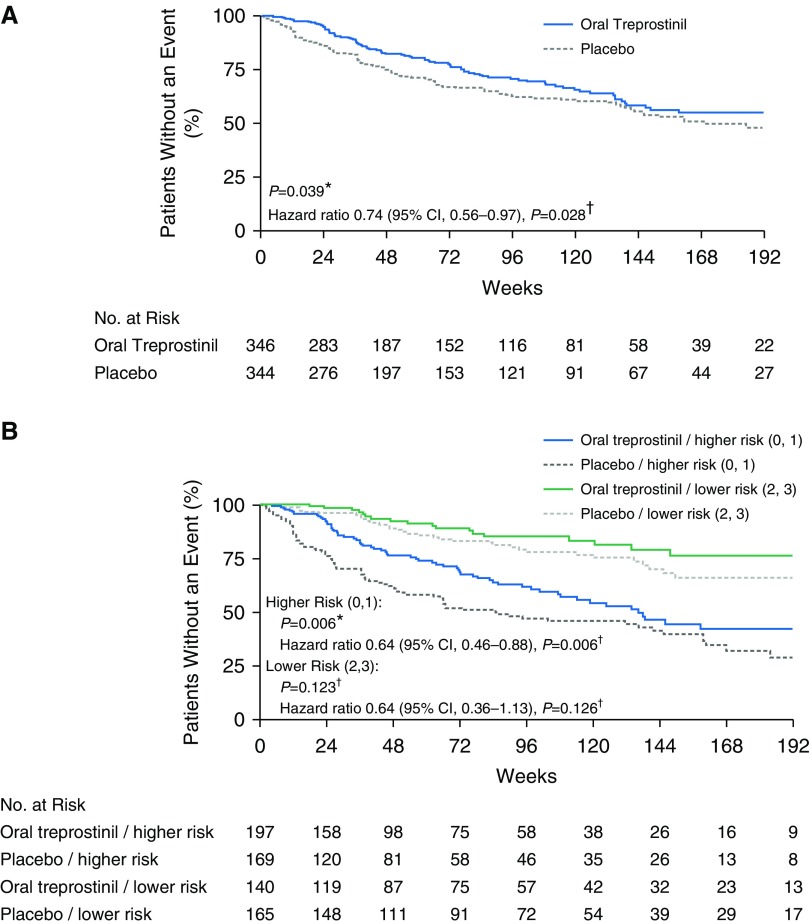
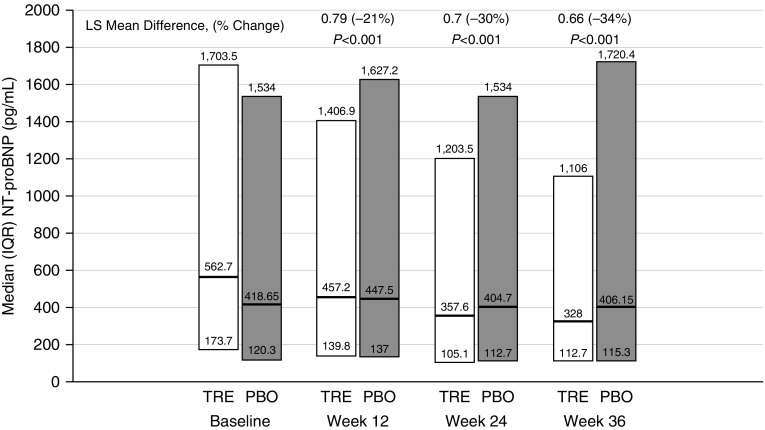
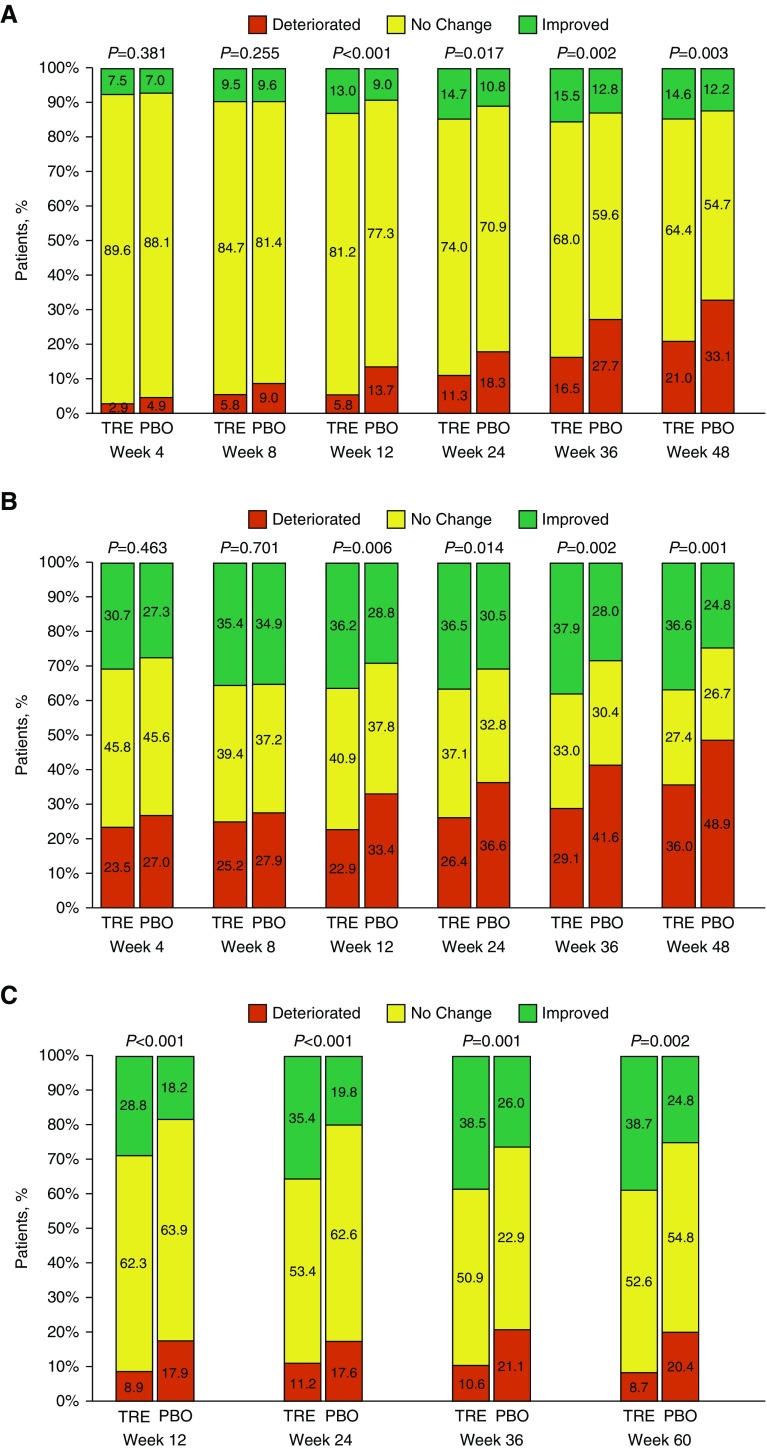
Rationale: Oral treprostinil improves exercise capacity in patients with pulmonary arterial hypertension (PAH), but the effect on clinical outcomes was unknown.Objectives: To evaluate the effect of oral treprostinil compared with placebo on time to first adjudicated clinical worsening event in participants with PAH who recently began approved oral monotherapy.Methods: In this event-driven, double-blind study, we randomly allocated 690 participants (1:1 ratio) with PAH to receive placebo or oral treprostinil extended-release tablets three times daily. Eligible participants were using approved oral monotherapy for over 30 days before randomization and had a 6-minute-walk distance 150 m or greater. The primary endpoint was the time to first adjudicated clinical worsening event: death; hospitalization due to worsening PAH; initiation of inhaled or parenteral prostacyclin therapy; disease progression; or unsatisfactory long-term clinical response.Measurements and Main Results: Clinical worsening occurred in 26% of the oral treprostinil group compared with 36% of placebo participants (hazard ratio, 0.74; 95% confidence interval, 0.56-0.97; P = 0.028). Key measures of disease status, including functional class, Borg dyspnea score, and N-terminal pro-brain natriuretic peptide, all favored oral treprostinil treatment at Week 24 and beyond. A noninvasive risk stratification analysis demonstrated that oral treprostinil-assigned participants had a substantially higher mortality risk at baseline but achieved a lower risk profile from Study Weeks 12-60. The most common adverse events in the oral treprostinil group were headache, diarrhea, flushing, nausea, and vomiting.Conclusions: In participants with PAH, addition of oral treprostinil to approved oral monotherapy reduced the risk of clinical worsening.Clinical trial registered with www.clinicaltrials.gov (NCT01560624).
Keywords: clinical study; combination therapy; oral treprostinil; pulmonary arterial hypertension; sequential therapy.
Figures
Comment in
-
An Event-driven Trial for Oral Treprostinil. Progress but Not the Holy Grail.Am J Respir Crit Care Med. 2020 Mar 15;201(6):647-649. doi: 10.1164/rccm.201912-2431ED. Am J Respir Crit Care Med. 2020. PMID: 31904994 Free PMC article. No abstract available.
References
-
- Humbert M, Lau EM, Montani D, Jaïs X, Sitbon O, Simonneau G. Advances in therapeutic interventions for patients with pulmonary arterial hypertension. Circulation. 2014;130:2189–2208. - PubMed
-
- Pulido T, Adzerikho I, Channick RN, Delcroix M, Galiè N, Ghofrani HA, et al. SERAPHIN Investigators. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013;369:809–818. - PubMed
-
- Sitbon O, Channick R, Chin KM, Frey A, Gaine S, Galiè N, et al. GRIPHON Investigators. Selexipag for the treatment of pulmonary arterial hypertension. N Engl J Med. 2015;373:2522–2533. - PubMed
-
- Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, Badesch DB, et al. Primary Pulmonary Hypertension Study Group. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med. 1996;334:296–301. - PubMed
-
- Jing ZC, Parikh K, Pulido T, Jerjes-Sanchez C, White RJ, Allen R, et al. Efficacy and safety of oral treprostinil monotherapy for the treatment of pulmonary arterial hypertension: a randomized, controlled trial. Circulation. 2013;127:624–633. - PubMed
