

RUBY-1: a randomized, double-blind, placebo-controlled trial of the safety and tolerability of the novel oral factor Xa inhibitor darexaban (YM150) following acute coronary syndrome
- PMID: 21878434
- PMCID: PMC3295208
- DOI: 10.1093/eurheartj/ehr334
RUBY-1: a randomized, double-blind, placebo-controlled trial of the safety and tolerability of the novel oral factor Xa inhibitor darexaban (YM150) following acute coronary syndrome
Abstract
Aims: To establish the safety, tolerability and most promising regimen of darexaban (YM150), a novel, oral, direct factor Xa inhibitor, for prevention of ischaemic events in acute coronary syndrome (ACS).
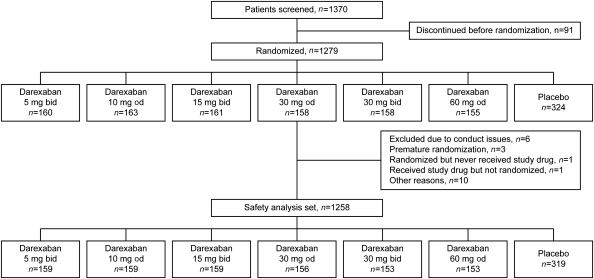
Methods: In a 26-week, multi-centre, double-blind, randomized, parallel-group study, 1279 patients with recent high-risk non-ST-segment or ST-segment elevation ACS received one of six darexaban regimens: 5 mg b.i.d., 10 mg o.d., 15 mg b.i.d., 30 mg o.d., 30 mg b.i.d., or 60 mg o.d. or placebo, on top of dual antiplatelet treatment. Primary outcome was incidence of major or clinically relevant non-major bleeding events. The main efficacy outcome was a composite of death, stroke, myocardial infarction, systemic thromboembolism, and severe recurrent ischaemia.
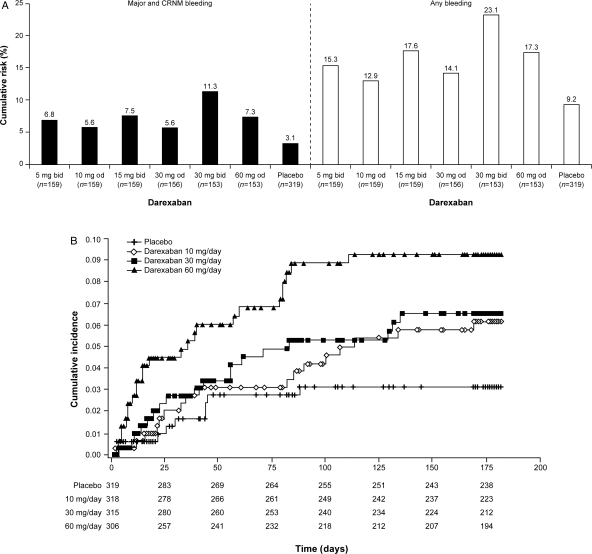
Results: Bleeding rates were numerically higher in all darexaban arms vs. placebo (pooled HR: 2.275; 95% CI: 1.13-4.60, P = 0.022). Using placebo as reference (bleeding rate 3.1%), there was a dose-response relationship (P = 0.009) for increased bleeding with increasing darexaban dose (6.2, 6.5, and 9.3% for 10, 30, and 60 mg daily, respectively), which was statistically significant for 30 mg b.i.d. (P = 0.002). There was no decrease (indeed a numerical increase in the 30 and 60 mg dose arms) in efficacy event rates with darexaban, but the study was underpowered for efficacy. Darexaban showed good tolerability without signs of liver toxicity.
Conclusions: Darexaban when added to dual antiplatelet therapy after ACS produces an expected dose-related two- to four-fold increase in bleeding, with no other safety concerns but no signal of efficacy. Establishing the potential of low-dose darexaban in preventing major cardiac events after ACS requires a large phase III trial. ClinicalTrials.gov Identifier: NCT00994292.
Figures
Comment in
-
On the cutting edge of acute coronary syndromes: adding oral factor Xa-inhibition with darexaban to dual antiplatelet therapy: the RUBY-1 trial.Eur Heart J. 2011 Oct;32(20):2486-8. doi: 10.1093/eurheartj/ehr314. Epub 2011 Aug 30. Eur Heart J. 2011. PMID: 21878435 No abstract available.
-
Acute coronary syndromes: Lackluster RUBY is received with some disappointment.Nat Rev Cardiol. 2011 Sep 20;8(11):610. doi: 10.1038/nrcardio.2011.145. Nat Rev Cardiol. 2011. PMID: 21931363 No abstract available.
References
-
- Fox KA, Steg PG, Eagle KA, Goodman SG, Anderson FA, Jr, Granger CB, Flather MD, Budaj A, Quill A, Gore JM GRACE Investigators. Decline in rates of death and heart failure in acute coronary syndromes, 1999–2006. JAMA. 2007;297:1892–1900. doi:10.1001/jama.297.17.1892. - DOI - PubMed
-
- Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, Falk V, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG, Tubaro M, Verheugt F, Weidinger F, Weis M ESC Committee for Practice Guidelines (CPG) Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: the task force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology. Eur Heart J. 2008;29:2909–2945. doi:10.1093/eurheartj/ehn526. - DOI - PubMed
-
- Bassand JP, Hamm CW, Ardissino D, Boersma E, Budaj A, Fernández-Avilés F, Fox KA, Hasdai D, Ohman EM, Wallentin L, Wijns W Task Force for Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of European Society of Cardiology. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes. Eur Heart J. 2007;28:1598–1660. doi:10.1093/eurheartj/ehm161. - DOI - PubMed
-
- Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC, Jr, Alpert JS, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK, Ornato JP. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction) J Am Coll Cardiol. 2004;44:E1–E211. doi:10.1016/j.jacc.2004.07.014. - DOI - PubMed
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE, Jr, Chavey WE, II, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Ornato JP, Page RL, Riegel B American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction); American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association of Cardiovascular and Pulmonary Rehabilitation; Society for Academic Emergency Medicine. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:e1–e157. doi:10.1016/j.jacc.2007.02.013. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
